Aviation Investigation Report A14O0077
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability.
Loss of control – Collision with water
Cessna 185E, C-FYKU
Taylor Lake, Ontario
Cessna 185E, C-FYKU
Taylor Lake, Ontario
Summary
On 24 May 2014, privately-registered Cessna 185E (registration C-FYKU, serial number 185-1484), equipped with amphibious floats, departed the Guelph Airpark for a flight to Taylor Lake, Ontario. The pilot was the sole occupant of the aircraft. While conducting a glassy water landing, the floats dug into the water, the pilot lost control, and the aircraft cartwheeled and sank. The aircraft fuselage was damaged by impact forces, and the pilot's door could not be opened.The pilot survived the impact but was not able to escape the submerged aircraft and drowned. The aircraft was equipped with an emergency locator transmitter which activated; however, no signal was received due to the antenna being submerged. The accident occurred during hours of daylight at approximately 0740 Eastern Daylight Time.
Le présent rapport est également disponible en français.
Factual information
History of the flight
The pilot flew several flights with another experienced pilot earlier in the month and during the week of the accident. The purpose of these flights was to practise landings and takeoffs after the winter break. During some of these flights, glassy-water landings were carried out. When practising glassy-water landings, the pilot would hunt or feel for the surface of the water by pitching the nose down without a reduction in engine power.The day before the occurrence, the pilot attempted to fly to Taylor Lake for a weekend of fishing with friends and family, but turned back due to weather en route.
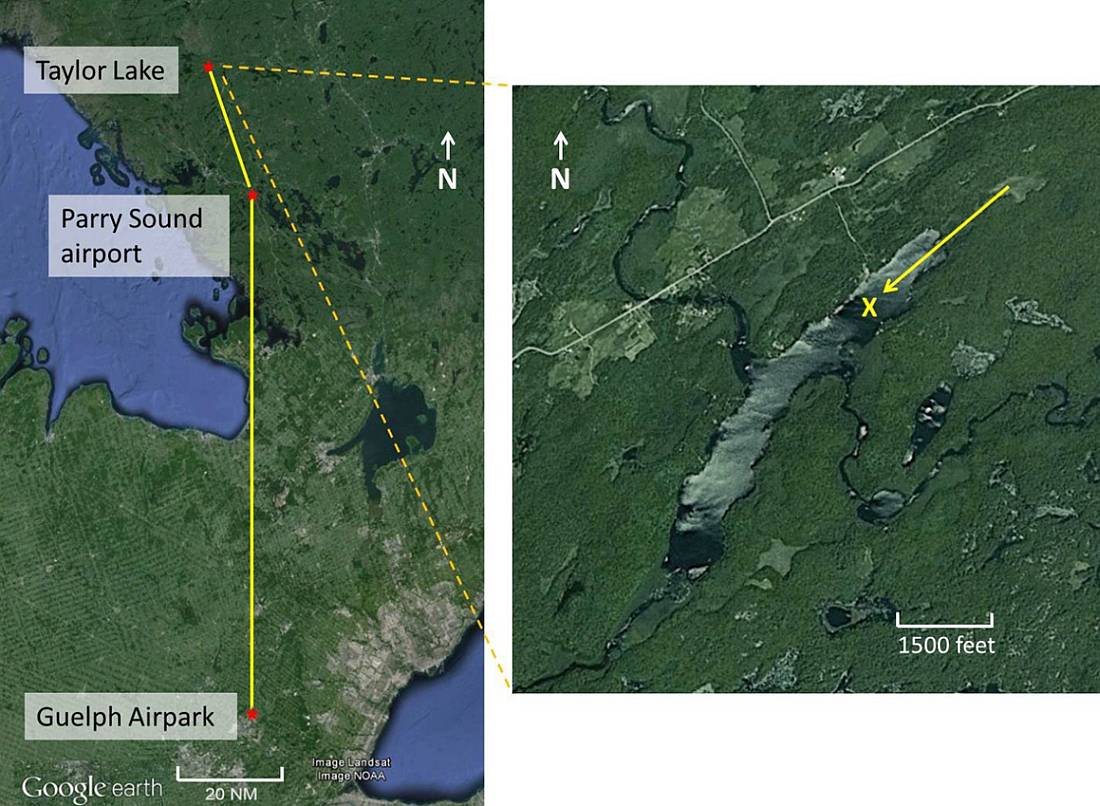
On the day of the occurrence, the pilot departed Guelph Airpark and flew to the Parry Sound Airport, Ontario, and conducted several touch-and-go landings on the runway prior to continuing on to Taylor Lake (Figure 1).
The aircraft touched down approximately level to the surface of the water with the right float slightly lower than the left. The floats then dug in causing the aircraft to cartwheel and flip inverted. The aircraft sank quickly and only the floats remained visible on the surface (Photo 1).
Bystanders immediately proceeded to the submerged aircraft and attempted to rescue the pilot, but were unable to open the doors and get the pilot out. Ontario Provincial Police divers recovered the pilot's body several hours later.

Weather
There was no aviation routine weather report (METAR) for Taylor Lake as the closest weather reporting station was located in North Bay (CYYB), Ontario, 50 nm to the north. The 0800 METAR for CYYB was as follows:Wind 350° True at 6 knots, visibility 15 statute miles, few clouds at 3000 feet above ground level (agl), few clouds at 12 000 feet agl, few clouds at 23 000 feet agl, temperature 14°C, dew point 6°C, and altimeter setting 30.12 inches of mercury.
Pilot
The pilot, who was in his seventies, held a private pilot licence – aeroplane, valid for single-engine, land and sea aircraft, as well as a valid category 3 medical certificate. The licence was originally issued on 23 March 1994. There was a restriction on the pilot's licence that correcting lenses must be worn, but the pilot was not wearing correcting lenses when recovered and none were found in the aircraft.The pilot had a pre-existing cardiac condition and was being treated by a cardiologist, and monitored in accordance with Transport Canada guidelines (Appendix C). The monitoring included regular resting electrocardiograms (ECG) and cardiac exercise stress testing, the results of which were within acceptable limits.
A TSB medical specialist reviewed the pilot's medical history. It was found that sublingual nitroglycerin spray, used to prevent or relieve chest pain (angina) in people with certain heart conditions, had been prescribed and that the pilot used a Continuous Positive Airway Pressure (CPAP) machine to treat sleep apneaFootnote 2. Neither had been reported to Transport Canada Civil Aviation Medicine (CAM) as required by Section 6.5 of the Aeronautics Act.
As well, the TSB medical specialist attended the post-mortem examination. During this examination, the pilot was found to have significantly more advanced cardiovascular disease than had been predicted; the major arteries were 80-90% blocked and posed a significant risk to the pilot. However, the pilot had passed the last required cardiac exercise stress test without any difficulty. The investigation concluded that the pilot's health state did not contribute to the accident.
The pilot's logbook was not recovered; however, the pilot reported having a total of 1300 total flying hours on his 2006 medical examination. The number of hours flown on the aircraft since the 2006 medical examination were obtained from the aircraft's technical logbooks. In the past several years, the pilot had accumulated only 53 flying hours.
- 2011: 24 hours
- 2012: 0 hours
- 2013: 29 hours
The pilot only flew during the spring, summer and autumn months, and was known for carefully planning flights and carrying the proper safety equipment on board at all times. The pilot was also known for diligently wearing the equipped lap and shoulder belt and a PFD while flying.
Aircraft
C-FYKU was manufactured in the United States by Cessna in 1969. The aircraft was equipped with EDO model 2790 amphibious floats when the pilot purchased it in October 1995, and had a total airframe time of 1736 hours.The journey logbooks were not recovered, but according to the technical log books, the last recorded maintenance was the annual inspection accomplished 19 July 2013, at a total airframe time of 2487 hours. According to available records, the aircraft was maintained in accordance with existing regulations. The aircraft was within weight and balance limitations.
The last Annual Airworthiness Information Report (AAIR) received by Transport Canada on 30 April 2014 showed that the aircraft had accumulated approximately 2516 hours total airframe time.
The 2 cabin doors served as the only available emergency exits. The door lock mechanism included a recessed lever-type exterior door handle that was flush with the door when closed, and a conventional L-shaped interior door handle. The Cessna 185 owner's manual Before Take-off Check List states that the cabin doors are to be locked during flight. Cessna indicated that the primary reason for locking the doors during flight is to prevent inadvertent opening due to fuselage flexure.
TSB Aviation Investigation Report A05O0147 included the following information with regards to door design:
By design, when the door is locked from the inside, it cannot be opened from the outside. Cessna indicated the following:The same design is currently being used in all new production single-engine Cessna aircraft.
As part of the aircraft design, testing and certification processes, safety issues relating to egress from the aircraft were considered at various stages. A variety of competing risks, safety factors and scenarios are evaluated through these processes. For example, risks associated with unexpected and/or unwanted opening of the doors are balanced against countervailing concerns such as access from outside the aircraft, with the goal being the development of a design that provides the best overall safety for the public.
Wreckage information
The following relevant facts were noted during the wreckage examination:- there was fuel on the water surrounding the aircraft;
- damage to both wing tips was consistent with a cartwheel;
- there were no anomalies with the aircraft flight controls;
- the flaps were in the 20-degree down position;
- there was no apparent damage to the floats or float attachments;
- the wheels were retracted;
- the propeller was completely detached from the engine, indicative of an engine operating with power at impact;
- the bottom of the left door was pushed partially into the cabin so that the door couldn't be opened;
- the left door handle was in the unlocked position;
- the left door window was found to be open; however, the window frame was bent, the window pane was broken and the lock was in the closed position;
- the bottom of the left wing was distorted and blocked the top of the left door so that it couldn't be opened;
- the right door and window handle were in the locked position;
- the windscreen was not broken and the V brace was not damaged;
- the pilot was not wearing the lap or shoulder harness when divers recovered the body;
- the baggage was not secured and was floating loosely within the cabin;
- the pilot was carrying sublingual nitroglycerin spray on his person and in his luggage; and
- a CPAP machine was found in the aircraft.
Survivability
There was minimal damage to the interior of the aircraft cabin, and the pilot survived the accident. The pilot's injuries consisted of minor abrasions and several broken ribs on the left side. The cause of death was drowning.The pilot was wearing a Mustang® inflatable personal flotation device (PFD) when he was recovered from the aircraft, but it was not inflated.
The TSB has investigated numerous seaplane accidents in which persons have survived the impact but were not able to safely egress from the aircraft (Appendix A). TSB Aviation Investigation Report A12O0071 states:
According to past research into accidents where helicopters were submerged in water, typically only 10% to 15% of people are able to carry out the required egress actions effectivelyFootnote 3. Another 10% to 15% of people typically fail to act from the extreme stress, greatly reducing their chance of survival. The remaining 75% may be stunned or shocked by the event; however, most are able to escape successfully if they are well trained and have rehearsed for such an event. Restrictions to normal exits, water temperature, darkness and disorientation following water impact further reduce the ability to egress. Escape training and passenger briefings emphasize the importance of memorizing exit locations.There is no record of the pilot receiving egress training, and there currently is no regulatory requirement for this type of training in private or commercial floatplane operations.
Over the years, the TSB has conducted numerous safety studies and issued Safety Recommendations, Aviation Safety Advisories and Safety Information Letters addressing egress issues and survivability in the seaplane industry. TSB Aviation Investigation Reports A09P0397 and A12O0071 highlight these safety communications issued by the TSB (Appendix B).
In the TSB Aviation Investigation Report A12O0071, to address egress issues in commercial seaplane operations, the Board recommended that :
The Department of Transport require underwater egress training for all flight crews engaged in commercial seaplane operations.In response to this recommendation, Transport Canada indicated that it will amend the current mandatory emergency training to include initial and recurrent underwater egress training for commercial flight crews. The new regulations have yet to be published. This action on the part of Transport Canada was assessed as Satisfactory Intent.
TSB Recommendation A13-02
Although steps have been taken by Transport Canada to address egress issues in the commercial seaplane industry, not much has been done over the years to address these same issues in the private seaplane community.
Glassy-water approach and landing
Although the pilot had experience landing on water, glassy-water conditions are considered to present the most difficulty for landing a seaplane, regardless of experience. The mirror effect created by glassy-water conditions affects depth perception making it difficult for pilots to determine the aircraft's height above the water.If glassy-water conditions exist, the Transport Canada Aeronautical Information Manual (TC AIM) recommends the followingFootnote 4:
Power assisted approaches and landings should be used although considerably more space will be required. The landing should be made as close to the shoreline as possible, and parallel to it, the height of the aircraft above the surface being judged from observation of the shoreline. Objects on the surface such as weeds and weed beds can be used for judging height. The recommended practice is to make an approach down to 200 feet (300 feet to 400 feet where visual aids for judgment of height are not available) and then place the aircraft in a slightly nose high attitude. Adjust power to maintain a minimum rate of descent, maintaining the recommended approach speed for the type until the aircraft is in contact with the surface. Do not “feel for the surface”. At the point of contact, the throttle should be eased off gently while maintaining back pressure on the control column to hold a nose high attitude which will prevent the floats from digging in as the aircraft settles into the water. Care must be taken to trim the aircraft properly to ensure that there is no slip or skid at the point of contact.
Analysis
The information obtained from the wreckage examination indicates that the engine was operating at the time of the accident and that there were no flight control anomalies that would have contributed to a loss of control. The minimal damage to the interior of the cockpit and the minor injuries received by the pilot indicate that this was a survivable accident. The analysis will examine the pilot's health, experience and inability to escape from the overturned aircraft.The number of hours the pilot had flown in recent years had decreased, and the pilot was likely less proficient than in earlier years, which would make the glassy-water landing more difficult.
The pilot was not wearing correcting lenses when recovered from the aircraft and no correcting lenses were found in the aircraft. It is possible the correcting lenses were lost during the accident and subsequent recovery, but not having the correcting lenses would have compounded the difficulty of a glassy-water landing.
The aircraft was configured properly for the landing and the approach was stable, indicating that the pilot was in full control of the aircraft up to the time of the accident.
Because landing an aircraft on glassy water can be very demanding, proper technique and landing attitude are critical to a successful glassy-water landing. The recommended procedure for landing is with a slight nose-high attitude, to prevent the floats from digging in on touchdown, and close to shore for better reference of height above the water. During the occurrence landing, the aircraft was in a nose-level attitude with the right float low just before touchdown in the centre of the lake.
The nose-level attitude at touchdown suggests that the pilot made contact with the lake unexpectedly, likely as a result of a lack of height references due to being so far from the shoreline and due to the glassy-water conditions. The floats dug in, which resulted in a loss of control and the aircraft cartwheeling.
The pilot was not wearing the lap belt and shoulder strap when recovered from the aircraft; however, based on previous history and habits it would have been out of character for the pilot not to be wearing them while flying the aircraft. Therefore, he survived with minor injuries, was able to release the lap belt and shoulder strap, and was able to unlock his door.
The impact forces were sufficient to cause airframe and door deformation rendering the pilot's door inoperable. The pilot's door window was damaged, but still functional and found to be open even though the window handle was in the locked position. It is not known when, how, or who opened the window, but egress could have been possible through the open window. The passenger door and window handles were both locked from the inside and had no damage.
Egress from one of these 2 points would have been possible if the pilot had unlocked either the passenger door or window. Rescuers were unable to assist the pilot as neither door would open from the outside. If rescuers are unable to open doors or windows from the outside, then there is a risk that the aircraft occupants will drown.
None of the baggage or equipment was restrained and was found to be floating all over the interior of the aircraft. This would have contributed to partially blocking any available egress path and would have contributed to an already confusing environment. Having survived the accident, the pilot was likely disoriented from a combination of factors, including the impact itself as well as being upside down, submerged in water, and surrounded by loose baggage.
Egress training has been shown to improve the chances of exiting a submerged aircraft following a survivable accident. However, there is no current requirement for this training in commercial or private operations. The pilot had not received any egress training and, as a result of the locked and jammed doors, disorientation and baggage blocking the egress points, he was unable to egress the aircraft, and drowned. If pilots operating seaplanes do not undergo egress training, there is an increased risk that they will be unable to escape from a submerged aircraft following a survivable accident.
The elderly pilot was given a valid category 3 medical certificate with a known cardiac condition that was being monitored and screened in accordance with existing Transport Canada guidelines. However, the post-mortem examination showed the pilot's condition was significantly more advanced than expected. The current screening processes, including the cardiac exercise stress test, did not detect the advanced state of the pilot's coronary heart disease. If medical screening tests do not accurately screen for advanced coronary heart disease, there is an increased risk that pilots could be flying with a condition that places people and property at risk of serious injury and death.
The pilot also had medication and a CPAP machine that were not reported to Transport Canada Civil Aviation Medicine (CAM). These overlooked items may have affected the decision by Transport Canada CAM to assess the pilot as fit for a category 3 medical certificate. If pilots and physicians do not report all medical conditions, then there is a risk that Transport Canada may not be able to properly assess the pilot's medical fitness.
Findings
Findings as to causes and contributing factors
- The number of hours the pilot had flown in recent years had decreased and the pilot was likely less proficient than in earlier years, which would make the glassy-water landing more difficult.
- The nose-level attitude at touchdown suggests that the pilot made contact with the lake unexpectedly, likely as a result of a lack of height references due to being so far from the shoreline and due to the glassy-water conditions.
- The right float contacted the water first, dug in, and resulted in a loss of control and the aircraft cartwheeling.
- The pilot had not received any egress training and, as a result of the locked and jammed doors, disorientation and baggage blocking the egress points, was unable to egress the aircraft, and drowned.
Findings as to risk
- If medical screening tests do not accurately screen for advanced coronary heart disease, there is an increased risk that pilots could be flying with a condition that places people and property at risk of serious injury and death.
- If pilots operating seaplanes do not undergo egress training, there is an increased risk that they will be unable to escape from a submerged aircraft following a survivable accident.
- If rescuers are unable to open doors or windows from the outside, then there is a risk that the aircraft occupants will drown.
- If pilots and physicians do not report all medical conditions, then there is a risk that Transport Canada may not be able to properly assess pilots' medical fitness.
Appendices
Appendix A – TSB aircraft accident investigation reports citing seaplane egress difficulties
| Occurrence | Type | Fatalities | Comments |
|---|---|---|---|
| A13O0125 | Cessna 182 | 3 | Two occupants were killed by impact forces. One occupant survived with minor injuries, but did not exit the aircraft, and drowned. |
| A12O0071 | DHC-2 Beaver | 2 | Two occupants of the aircraft were seriously injured due to the lack of effective restraints. These injuries rendered them unconscious and they were unable to survive the post-crash water environment. One occupant received injuries and was able to egress successfully. |
| A09P0397 | DHC-2 Beaver | 6 | Because of impact damage, only 2 of the 4 exits were usable following the crash. Five of the 6 persons who drowned removed their seatbelts after the impact, which indicates that they survived the impact, but were unable to locate a suitable egress point. The TSB published recommendations A11-05 and A11-06 following this report. |
| A05O0147 | Cessna 185F | 1 | In this occurrence, the pilot drowned. The Board indicated its concern as follows: “Based on historical data, occupants of submerged seaplanes who survive the accident continue to be at risk of drowning inside the aircraft. Existing defences against drowning in such circumstances may not be adequate. In light of the potential loss of life associated with seaplane accidents on water, the TSB is concerned that seaplane occupants may not be adequately prepared to escape the aircraft after it becomes submerged. Of equal concern is that the rescuers, in this occurrence, could not access the cabin from outside.” |
| A05Q0178 | Cessna 185 | 1 | After the aircraft capsized while attempting to take off, 5 occupants were able to escape. One occupant, seated in the front right seat, was unable to escape the submerged cabin and drowned. |
| A04W0114 | Cessna 185F | 2 | The survivors were unable to locate the interior door handles after the seaplane became inverted and submerged in the water, thus preventing them from using the doors as emergency exits. The TSB report presented the following Board concern: “Based on historical data, occupants of submerged seaplanes who survive the accident continue to be at risk of drowning inside the aircraft. Existing defences against drowning in such circumstances may not be adequate. In light of the potential loss of life associated with seaplane accidents on water, the TSB is concerned that seaplane occupants may not be adequately prepared to escape the aircraft after it becomes submerged. The Board is also concerned that seaplanes may not be optimally designed to allow easy occupant egress while under water.” |
| A03F0164 | Cessna 185 | 1 | One passenger was unable to escape from the aircraft and drowned. |
| A03Q0083 | Cessna U206F | 1 | The pilot exited the aircraft and told the passenger to follow. The passenger, disoriented, went to the rear of the aircraft and drowned. |
| A00P0103 | DHC-2 Beaver | 3 | In this fatal occurrence, the aft centre of gravity contributed to the cause of the accident. This aircraft had no stall warning system. Two passengers were unable to escape the aircraft and another drowned while attempting to swim to shore. |
| A98P0215 | DHC-2 Beaver | 5 | All 5 occupants drowned following a survivable impact with water. Medical information revealed that the occupants had been restrained during the initial impact and rollover. |
| A97P0230 | Cessna 180J | 3 | All 3 occupants drowned following a survivable impact with water. |
| A97C0090 | Cessna TU206G | 2 | The 2 passengers were unable to exit the aircraft and drowned. |
| A96Q0114 | Cessna U206F | 4 | The pilot and 3 passengers drowned inside the aircraft. Prior to this occurrence, the Canadian Aviation Safety Board forwarded an Aviation Safety Advisory to Transport Canada indicating that the rear double cargo door of the Cessna 206 was hard to open. No measures were taken to have the doors modified. |
| A94O0213 | Cessna A185E | 3 | One passenger was able to exit the aircraft through the left door window and swim to shore. The pilot and the other 2 passengers did not survive. Both doors remained closed throughout the impact, but both side door windows were fully open when the aircraft was located. |
| A91Q0267 | Cessna A185F | 2 | The handle of the right door was broken; however, the passenger occupying the right front seat managed to exit the aircraft through the window of the right door. The pilot and rear seat passenger, who had no signs of physical trauma on their bodies, drowned. |
| A91C0122 | DHC-2 Beaver | 1 | The pilot survived the impact, but drowned while trying to escape from the wreckage. |
| A90W0265 | DHC-2 Beaver | 2 | One passenger was able to exit the aircraft; however, the pilot and second passenger did not, and drowned. Damage to the wings blocked both right doors and the left cabin door. |
| A89O0369 | Cessna TU206G | 1 | The pilot exited the aircraft by kicking open the port-door window. However, there was no door beside the front passenger; that passenger was unable to egress and drowned. |
| A89C0089 | Cessna A185 | 1 | One of the 4 occupants was trapped in the aircraft and drowned. |
| A88O0203 | DHC-2 Beaver | 2 | The pilot and front-seat passenger were unable to escape from the sinking aircraft and drowned. |
| A87P0901 | Cessna 180J | 1 | The pilot was able to escape from the submerged aircraft through the left door. He then repeatedly dove underwater in an attempt to rescue the other occupant, but was unable to locate her. She was found by rescuers at the rear of the cabin 20 minutes later, but died in hospital several days after the accident. Neither occupant suffered incapacitating injuries during the crash sequence. |
| A87P0021 | Cessna A185F | 1 | The pilot was unable to escape from the submerged aircraft and drowned. |
| A86P0058 | DHC-2 Beaver | 5 | The pilot escaped with serious injuries and 5 passengers drowned. The report highlighted that, when the centre seat is installed, the rotary knob for opening the rear door is located behind the seat. As such, the door cannot easily be opened by passengers sitting in the centre seat. |
Appendix B – TSB safety studies and safety communications related to floatplane and seaplane safety
- A Safety Study of Piloting Skills, Abilities, and Knowledge in Seaplane Operations (TSB report number SSA93001): This 1993 study examined 1432 seaplane accidents. Although the study did not focus on survivability issues, it did compare the ratio of fatal accidents to total accidents for float-equipped aircraft to that of wheel-equipped aircraft (for those makes and models of aircraft most frequently float-equipped). When these aeroplanes were on wheels, 10% of the accidents were fatal. However, when they were on floats, 17% were fatal. In the study, 10 safety recommendations aimed at reducing the number of seaplane accidents.
- A Safety Study of Survivability in Seaplane Accidents (TSB report number SA9401): This 1994 TSB safety study analyzed seaplane accidents in Canada over the fifteen-year period from 1976 to 1990. During that time, there were 1432 such accidents, of which 234 resulted in 452 fatalities. The safety study contained 6 recommendations to enhance the survivability of persons involved in seaplane accidents, including a recommendation on wearing personal flotation devices during the standing, taxiing, takeoff, approach, and landing phases of flight (TSB Recommendation A94-07).
- TSB Safety Advisory A000003-1, Escape from a Submerged Seaplane: The TSB issued this safety advisory following an accident in 2000 involving a de Havilland DHC-2 Beaver. Amongst other things, the safety advisory suggested that quick release mechanisms or push-out windows would enhance rapid egress. Transport Canada (TC) did not, however, implement requirements for these modifications to floatplanes.
- TSB Safety Advisory A040044-1, Egress from Submerged Seaplanes: The TSB issued this safety advisory following a 2004 accident involving a Cessna A185F seaplane carrying 1 pilot and 3 passengers. In this occurrence, the pilot and the right front-seat passenger were unable to open either of the main exits and egressed through the broken window in the left cabin door. The 2 rear-seat passengers drowned, despite the fact that they had not sustained any physical injuries during the occurrence. The advisory stated that modifications to seaplane doors to provide a quick release mechanism or the fitting of pop-out windows would enhance the opportunity for rapid egress in the event that the aircraft becomes submerged. The advisory suggested that TC may wish to consider additional methods to facilitate rapid emergency egress from seaplanes in the event that the cabin becomes submerged. In its response, TC indicated that jettisonable doors and large frangible or pop-out windows that would facilitate emergency exits is within the authority of the state of design authority, and that TC would not take any action relating to this issue.
- TSB Aviation Safety Information Letter A040046, Passenger Briefings and Safety Features Cards in Seaplane Operations: This information letter was produced following the 2004 accident involving a Cessna A185F seaplane cited in the previous paragraph. The information letter highlighted that the regulations were not instructive with regard to a requirement for the briefing to include information specific to underwater egress procedures in seaplane operations. Furthermore, there is no requirement for seaplane safety feature cards to contain information or special procedures unique to underwater egress. The information letter concluded by highlighting that the risks associated with seaplane passengers and pilots being trapped inside a submerged aircraft are increased when the pre-flight safety briefing and the safety features cards do not include information specific to underwater egress. In its response, TC advised that it sent 100 copies of its revised brochure entitled Seaplanes – A Passenger's Guide (TP 12365) to every commercial seaplane operator in Canada, with instructions on how to order more if needed.
Appendix C – Acute ischemic syndrome
Source: Source: Transport Canada, Handbook for Civil Aviation Medical Examiners (TP 13312E), 2004, p. C-4Acute Ischemic Syndrome
An acute ischemic syndrome is initially incompatible with medical certification. However, disqualification is not necessarily permanent, and medical certification may be considered 6 months after the event (a decision at 6 months must be based on requisite assessments completed no sooner than 5 months after discharge from hospital) provided the following criteria are met:
- The result of an exercise test to a minimum of 8.5 METS (end of Stage 3) using the Bruce protocol or equivalent places the individual at low (<2%) risk of a significant cardiovascular event over the following 12 months. Medications need not be stopped for these tests. If a perfusion exercise test is used, there should be no significant reversible defect and no large fixed deficit as explained in the next point.
- The left ventricular ejection fraction as a measure of left ventricular function using echocardiography or gated radionuclide scintigraphy, is better than 50% at rest and does not show a decrease of more than 5% with satisfactory exertion (i.e. 85% predicted maximum heart rate or > 8 METS). A threshold ejection fraction of 45% applies with the use of SPECT (single proton emission computerized tomography) scanning.
- With a satisfactory ejection fraction as described above, Holter monitoring is not required. For an ejection fraction between 40% and 50%, restricted medical certification may be considered after review of a 24 hour Holter monitor. This should reveal no more than 3 ventricular ectopic beats per hour in the absence of antiarrhythmic medication, with no more than 3 consecutive beats and a cycle length that is not less than 500 msec.
- Major modifiable risk factors (see below) for recurrence of infarction are controlled, and the applicant is a non-smoker.
- A follow-up assessment a year after the infarction and then annually should include a thorough history, physical examination, rest and exercise electrocardiography and a review of modifiable risk factors. If there is no clinical deterioration after 2 years, the treadmill exercise test can be done every 2 years until the applicant is 50 years of age and subsequently the possible need for yearly testing should be considered.
- These criteria apply regardless of whether the applicant was treated for acute thrombosis e.g., with a thrombolytic drug, percutaneous coronary intervention (PCI) or bypass surgery, or the infarction occurred in the presence of only mild to moderate atheromatous disease as demonstrated by arteriography.
Following Revascularization
An applicant who has been treated for coronary artery disease by revascularization including bypass surgery, angioplasty with or without stenting, directional atherectomy etc., can be considered for medical certification after an interval of 6 months, provided the following criteria are met:
- The result of an exercise test to a minimum effort of 8.5 METS (end of Stage 3) using the Bruce protocol or equivalent places the individual at low (<2%) risk of a significant cardiovascular event over the following 12 months.
- Patency of the revascularized artery is maintained with no evidence of reversible ischemia on rest and exercise perfusion imaging.
- Major modifiable risk factors (see below) are controlled and the applicant is a non-smoker.
- Left ventricular function following bypass surgery is satisfactory.
- A follow-up assessment a year after the revascularization and then annually should include a thorough history, physical examination, rest and exercise electrocardiography and a review of modifiable risk factors. If there is no clinical deterioration after 2 years, the treadmill exercise test can be done every 2 years until the applicant is 50 years of age and subsequently the possible need for yearly testing should be considered.
Footnotes
- Footnote 1
- All times are Eastern Daylight Time (Coordinated Universal Time minus 4 hours)
- Footnote 2
- Sleep apnea is a potentially serious sleep disorder in
which breathing stops and starts. People with the disorder are at
increased risked of having a cardiac event (Source: Mayo Clinic Staff,
Diseases and Conditions, Sleep Apnea, 24 July 2012).
- Footnote 3
- C.J. Brooks, C.V. MacDonald, L. Donati and J.T. Taber,
“Civilian Helicopter Accidents into Water: Analysis of 46 Cases,
1979–2006,” Aviation, Space, and Environmental Medicine, Vol. 79, No. 10 (2008), pp. 935–940.
- Footnote 4
- Transport Canada Aeronautical Information Manual, AIR 2.11.4, 16 October 2014.