Aviation Investigation Report A12Q0216
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability.
Low-energy rejected landing and collision with terrain
Perimeter Aviation LP
Fairchild SA227-AC Metro III, C-GFWX
Sanikiluaq, Nunavut
Perimeter Aviation LP
Fairchild SA227-AC Metro III, C-GFWX
Sanikiluaq, Nunavut
Summary
On 22 December 2012, the Perimeter Aviation LP, Fairchild SA227-AC Metro III (registration C-GFWX, serial number AC650B), operating as Perimeter flight PAG993, departed Winnipeg/James Armstrong Richardson International Airport, Manitoba, at 1939 Coordinated Universal Time (1339 Central Standard Time) as a charter flight to Sanikiluaq, Nunavut. Following an attempted visual approach to Runway 09, a non-precision non-directional beacon (NDB) Runway 27 approach was conducted. Visual contact with the runway environment was made and a circling for Runway 09 initiated. Visual contact with the Runway 09 environment was lost and a return to the Sanikiluaq NDB was executed. A second NDB Runway 27 approach was conducted with the intent to land on Runway 27. Visual contact with the runway environment was made after passing the missed approach point. Following a steep descent, a rejected landing was initiated at 20 to 50 feet above the runway; the aircraft struck the ground approximately 525 feet beyond the departure end of Runway 27. The 406 MHz emergency locator transmitter activated on impact. The 2 flight crew and 1 passenger sustained serious injuries, 5 passengers sustained minor injuries, and 1 infant was fatally injured. Occupants exited the aircraft via the forward right overwing exit and were immediately transported to the local health centre. The aircraft was destroyed. The occurrence took place during the hours of darkness at 2306 Coordinated Universal Time (1806 Eastern Standard Time).Le présent rapport est également disponible en français.
1.0 Factual information
1.1 History of the flight
On 22 December 2012, the Fairchild SA227-AC Metro III,Footnote 1 operated under instrument flight rules (IFR)Footnote 2 as Perimeter flight PAG993, was chartered for a flight from Winnipeg/James Armstrong Richardson International Airport (CYWG), Manitoba, to Sanikiluaq (CYSK), Nunavut. The charter flight was operated under Subpart 704 of the Canadian Aviation Regulations (CARs).Footnote 3 This route is normally operated by Keewatin Air, a Perimeter Aviation LP (Perimeter) sister company,Footnote 4 every Monday, Wednesday and Friday. The normally scheduled flight on the previous day (Friday, 21 December 2012) had been cancelled due to poor weather in CYSK. With extra cargo and passengers needing to travel to CYSK before Christmas, Keewatin Air completed a flight on the morning of 22 December 2012 and had chartered Perimeter to complete an additional flight. The Perimeter flight crew had been notified in the early evening of 21 December 2012 that they would be operating flight PAG993 the next morning.Upon arriving at the airport at approximately 1330 Coordinated Universal Time (UTC),Footnote 5 the captain checked the weather on the NAV CANADA aviation website and filed the flight plan with Winnipeg flight information centre (FIC). The 3-hour IFR flight was initially flight planned to depart at 1530 UTC. The chosen alternate aerodromeFootnote 6 was Moosonee (CYMO), Ontario. Perimeter does not operate scheduled flights to CYSK. As there were several MEDEVAC and charter flights to areas in Nunavut that day, there was an insufficient number of available instrument approach charts for Nunavut at the flight planning/flight following office during pre-flight planning. It was arranged that a set of charts would be picked up at Keewatin Air prior to departure.
The first officer (FO) reported to work at 1345 UTC and inspected the aircraft. As no survival kit was on board and was necessary as per company procedure,Footnote 7 the captain was advised and one was requested. There were several flights to the North taking place that day, and Perimeter did not have a survival kit available for the CYSK flight. It was arranged to have one supplied by Keewatin Air and it was obtained prior to departure. During inspection of the aircraft, it was noticed that the cargo door unsecure warning light remained illuminated; maintenance was advised, the cargo door handle position switch was replaced, and the aircraft returned to service approximately 3 hours later.
Following completion of the maintenance work, the captain checked the actual weather, aerodrome and area forecasts for the takeoff, en-route, destination, alternate and return trip segments again (see Section 1.7 Meteorological information), and filed a new flight plan, with a planned departure time of 1930 UTC. After taxiing from the Perimeter ramp to the Keewatin Air ramp, freight and fuel were loaded, and passengers embarked. Due to additional freight added, less fuel could be carried. Therefore, the planned alternate airport was changed to Kuujjuarapik (CYGW), Quebec, situated 90 nautical miles (nm) southeast of CYSK.
The weight and balance/loadsheet indicated that the take-off weight from CYWG to CYSK was 15 993 pounds, which is just below the aircraft maximum allowable take-off weight of 16 000 pounds. However, an additional 200 pounds of fuel had been loaded which did not appear on the loadsheet. At normal consumption rates, the fuel load declared would provide 5 hours of fuel on board. The extra 200 pounds of fuel would allow for an additional 20 minutes of flight.
The FO briefed the passengers on the use of seatbelts and location of emergency exits. Although required by regulations, no individual safety briefing was given to a mother holding her infant;Footnote 8 she was seated in the first seat on the left, seat 1L, next to the main door. There was no assigned seating; passengers chose their own seat. The mother of the infant was not directed to sit elsewhere.
PAG993 departed at 1939 UTC, 4 hours later than originally planned. The captain was seated in the left seat and was the pilot not flying (PNF). The FO was seated in the right seat and was the pilot flying (PF) out of CYWG. Shortly after departure, the captain realized that the instrument approach charts for CYSK had been forgotten.
The captain chose not to return to CYWG to obtain the instrument approach charts as this would delay the flight even more and add to the crew duty day. Instead, he obtained chart information pertaining to the non-directional beacon (NDB) Runway 27 instrument approach for CYSK via radio from a company pilot (Appendix A). Information obtained did not include the direction for the procedure turn or the minimum descent altitude (MDA)(620 feet above sea level [asl]) for the circling approach to Runway 09.
The take-off, climb and cruise segments of the flight were uneventful, with the exception of light turbulence for which the crew requested a climb to FL230.Footnote 9 Flying duties were shared for the cruise portion of the 3-hour flight. Weather condition updates and forecasts for destination and alternate airports were not verified until just prior to descent.
When the aircraft was 82 nm to the west of CYSK, just before starting descent, the crew contacted the community aerodrome radio station (CARS) observer/communicator for the latest weather and runway surface condition (RSC) for CYSK. The crew also requested weather for CYSK and CYGW with Quebec Radio. CYGW, the flight-planned alternate airport, showed weather to be worse than what was obtained prior to departure. Due to the poor weather conditions at CYGW, weather for La Grande Rivière airport (CYGL), Quebec, located 260 nm south-southeast of CYSK, was also obtained.
The crew discussed the remaining fuel on board and determined they would not have enough fuel for CYGL plus the required reserve;Footnote 10 CYGL was therefore discarded as an alternate airport option. There was sufficient fuel on board to conduct several approaches at CYSK before needing to consider diverting to CYGW. Given the weather, there was doubt as to whether a diversion to the alternate airport was practical. CYSK has a gravel runway, and company procedures require that landing on gravel runways be conducted by the captain;Footnote 11 therefore, the captain assumed PF duties. The FO was designated as PNF.
Appendix B shows a compilation of all flight trajectories during the attempted landings at CYSK. The aircraft arrived from the west, and the wind direction was slightly left of the arrival track. There is no published instrument approach for Runway 09 at CYSK. The crew's plan was to descend to the minimum safe altitude (MSA) of 1600 feet asl and, if the runway environment for landing Runway 09 could be seen, then a straight-in visual approach Runway 09 would be executed (Figure 1).

The reference speed (VREF)Footnote 12 for the approach and landing was 113 knotsFootnote 13 plus consideration for wind gusts, resulting in a target speed of 118 knots to cross the threshold. The crew rounded this off to 120 knots. At 2240 UTC, the weather at CYSK was reported as: wind 040° magnetic (M) at 15 knots gusting to 20 knots, altimeter setting 29.24 inches of mercury (in. Hg).
The runway environment for landing straight-in Runway 09 was not visible while flying inbound to the YSK NDB at 1600 feet asl. After passing the YSK NDB at 2244 UTC, the aircraft proceeded outbound to complete the full procedure turn for the NDB Runway 27 approach (Figure 2). The procedure turn is published to be executed on the north side of the approach track at 1400 feet asl.
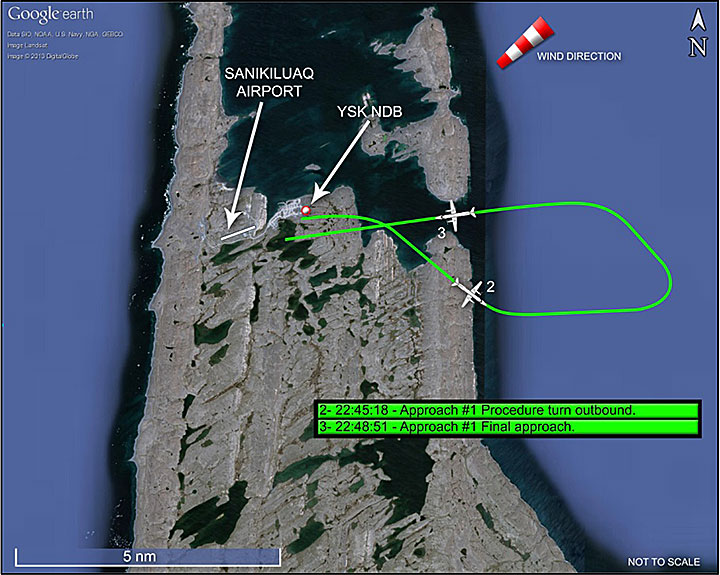
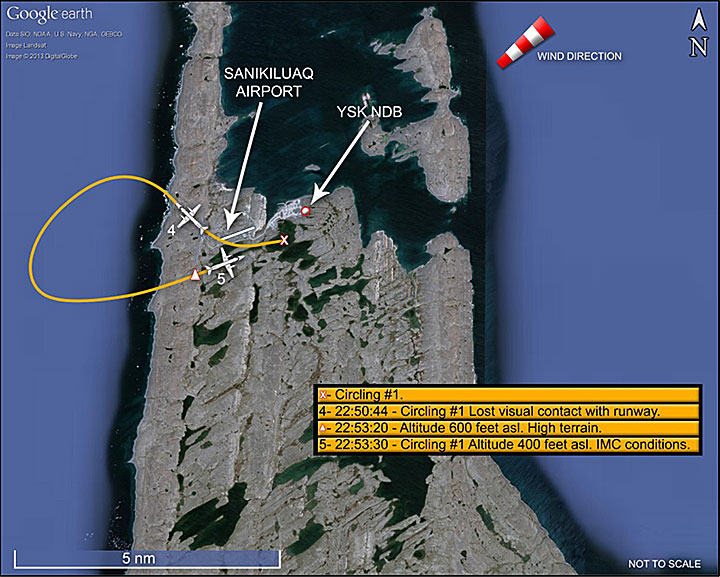
The lights of the town, situated just over 0.6 nm east of the airport, were observed while the aircraft was on final approach; the crew could not see the runway environment. Visual contact with the runway environment was made approximately 0.6 nm from the threshold of Runway 27 at an indicated altitudeFootnote 14 of 600 feet. The published MDAFootnote 15 is 560 feet asl; the published minimum circling altitude of 620 feet asl had not been obtained and therefore not used. A left-hand circling for Runway 09 was initiated. The aircraft descended to an indicated altitude of approximately 500 feet. Thirty seconds later, at 2251 UTC, visual contact with the ground was lost, and the circling manoeuvreFootnote 16 was continued in instrument meterological conditions (IMC). A go-aroundFootnote 17 was not called or initiated, and the published missed approach procedure was not followed.
At 2253 UTC while continuing to circle in IMC, the aircraft descended to an indicated altitude of 400 feet, at a speed of 140 knots. The wind was pushing the aircraft south of the Runway 09 centreline in an area southwest of the runway where the terrain elevation is 223 feet asl, resulting in a height of 155 feet above ground level (agl) when applying cold temperature corrections (Figure 3).Footnote 18
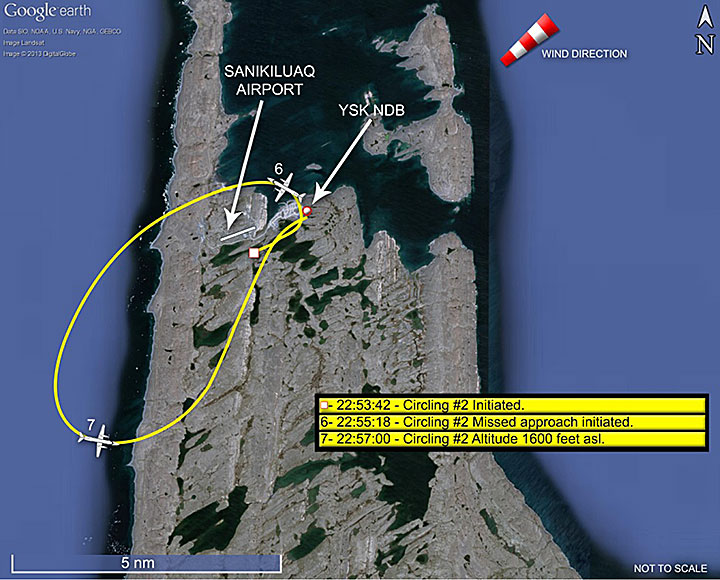
The captain indicated this would be the last attempt at landing at CYSK. They would then proceed to the flight-planned alternate, CYGW, approximately 30 minutes away. Fuel at this time was 1000 pounds, giving approximately 1.6 hours of flight. The full procedure turn was once again flown on the opposite side of the published procedure, this time at an indicated altitude of 1500 feet (1389 feet asl when applying cold temperature corrections), 211 feet below the published MSA of 1600 feet asl (Figure 5).
For this approach, the GPS was used to carry out the NDB RWY 27 (GNSS)Footnote 21 overlay approach, to navigate towards the airport. The GPS was set up to navigate to the airport reference point, located at the centre point of the runway, to provide the crew with the approximate distance of the aircraft from the threshold of Runway 27 and more precise tracking to the airport (Appendix C).
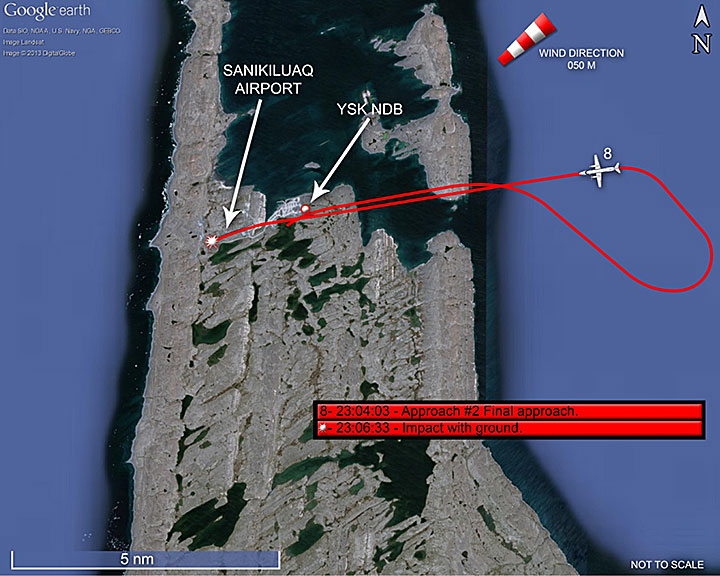
The before landing checklist was completed prior to interception of the final approach path for Runway 27. At 2302:36 UTC, the FO reported the aircraft position as procedure turn inbound. The CARS observer/communicator acknowledged the position report, and provided the wind and visibility (1½ statute miles [sm]). The aircraft was established at an indicated altitude of 400 feet, 3 nm from the airport, 197 feet below the published MDA, without having established the required visual references.Footnote 22
At 2305:57 UTC, the crew acquired visual contact with the runway at 400 feet indicated, just beyond the missed approach point (MAP), at approximately 0.7 nm from the threshold of Runway 27. Full flaps were selected for landing, power decreased to idle, and the descent was initiated at 2306:07 UTC. The speed was 140 knots (Appendix D).
The ground proximity warning system (GPWS) generated a SINK RATE warning at 2306:11 UTC as the rate of descent exceeded 1500 feet per minute (ft/min), followed by a PULL UP warning at 2306:13 UTC as the rate of descent exceeded 1800 ft/min. The PULL UP-PULL UP warning sounded 3 times over a 4-second period. The first PULL UP warning occurred as the aircraft was approximately 200 feet from the threshold of the runway, at a height of approximately 180 feet agl and a speed of 145 knots (estimated 159 knots ground speed). The last warning at 2306:17 UTC, occurred approximately 900 feet past the threshold, at approximately 60 feet agl. The high rate of descent was reduced over the runway. At 2306:21 UTC, the aircraft passed the runway midpoint in a nose-up attitude at a height of approximately 20 to 50 feet agl with a speed of 125 knots resulting in a ground speed of approximately 135 knots. Two seconds later, the captain called for a go-around, engine power was increased, gear retracted and flaps set to the ¼ position setting. At that time, the aircraft was approximately 2300 feet beyond the Runway 27 threshold.
At 2306:29 UTC, the FO called the speed at 105 knots.Footnote 23 At 2306:33 UTC, the aircraft collided with terrain beyond the departure end of Runway 27 and south of the runway centreline. The aircraft continued to slide and rotate right, before coming to rest on an easterly heading. The FO initiated the evacuation. The forward right overwing window emergency exit was used to exit the aircraft. The captain made a mayday call on the CYSK radio frequency. Airport employees, family members and other villagers awaiting the aircraft's arrival immediately responded to the occurrence. All occupants were transported to the community health centre. The quick response of the people on the ground reduced the exposure of passengers and crew to the elements. The flight crew were flown to Winnipeg for medical care the following day.
1.2 Injuries to persons
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | - | 1 | – | 1 |
| Serious | 2 | 1 | – | 3 |
| Minor/None | – | 5 | – | 5 |
| Total | 2 | 7 | – | 9 |
1.3 Damage to aircraft
The doors of all 3 landing gear bays were open on impact and were torn away, indicating that the gear was in transition when the aircraft struck the ground, but not yet fully up and locked. The right main gear and the nose landing gear were torn away on impact with the ground. The left main gear was found retracted into the gear well; however, the tires were cut and bruised; the left main gear retracts slightly ahead of the right gear in normal operation. The landing gear selector in the cockpit was found in the UP position.Both propellers had broken away from the engine propeller shafts close to the initial impact point. The propeller blades were severely distorted and several had separated from the propeller hubs. The damage sustained by the propellers indicated that both engines were producing significant power at the time of impact.
The fuselage belly skin and underside of the engines were cut and ripped open while sliding across the sharp, rocky terrain, exposing wire bundles, hoses, insulation, lines, and buckling the floor. The fuselage fractured at the forward pressure bulkhead and in the rear baggage compartment area below the dorsal fin. Snow and gravel entered the cockpit floor areas via the openings in the floor and fuselage. Both wings remained attached to the fuselage, but were substantially damaged. There was no post-impact fire (Photo 1).

1.4 Other damage
With the exception of minor oil spillage from the engines, there was no damage to property or the environment.1.5 Personnel information
1.5.1 Flight crew
1.5.1.1 General
Based on available records, the pilots were certified and qualified for the flight in accordance with existing regulations.| Captain | First officer | |
|---|---|---|
| Pilot licence | ATPL (airline transport pilot licence) | CPL (commercial pilot licence) |
| Medical expiry date | 01 April 2013 | 01 May 2013 |
| Total flying hours | 5700 | 1250 |
| Hours on type | 2330 | 950 |
| Hours in the last 7 days | 18 | 14 |
| Hours in the last 30 days | 63 | 45 |
| Hours in the last 90 days | 144 | 153 |
| Hours on type in the last 90 days | 144 | 153 |
| Hours on duty prior to the occurrence | 9.5 | 9.5 |
| Hours off duty prior to the work period | 48 | 9.5 |
1.5.1.2 Captain
The captain was hired by Perimeter in May 2006 as FO on the Fairchild SA226-AC Metro II and the Fairchild SA227-AC Metro III. In April 2007, he was awarded a captain position on the Metro II, and on the Metro III in January 2008. In August 2008, he went on to work with a large air carrier overseas as FO on heavy jet aircraft. In March 2009, the captain flew large turboprop aircraft for a Canadian Subpart 705 operator initially as FO, then as captain. In June 2011, he flew as FO on heavy jet aircraft with a different Canadian air carrier. His departure from that company was precipitated by a layoff of flight crew. In October 2012, the captain returned to Perimeter to fly as captain on the Metro III.During his previous years of employment with Perimeter, the captain had gained experience flying in the North. Since being rehired, he had been to CYSK twice before the day of the occurrence, once by day and once by night. Visual meteorological conditions (VMC) had prevailed on both occasions. As captain, he was authorized to land on gravel surface runways.
For the 7-day period prior to the occurrence, the captain had flown a total of 18 hours with a total duty time of 34.4 hours for that period. The captain was off duty the 2 days preceding 22 December. He had a fairly good sleep the night before reporting for duty; he woke once and had taken 1.5 hours before falling back to sleep but eventually managed to do so. He felt rested prior to beginning the work shift. He had been on duty for approximately 9.5 hours when the occurrence took place.
The originally planned total duty day, including the return trip, would normally have taken approximately 9.5 hours. Because of the delays incurred, the flight crew's duty day was extended. Had the delayed flight landed without incident at CYSK and the aircraft flown back to Winnipeg as planned, the duty day for both crew members would have been approximately 14 hours.Footnote 24
1.5.1.3 First officer
The FO began employment with Perimeter as a ramp worker while he completed his multi-engine and instrument ratings. He commenced duty as FO on the Metro III in July 2011. The FO had flown to CYSK once before the previous summer, by day, in VMC. As FO, he was not authorized to land on gravel surface runways. In the 72 hours prior to the occurrence, the FO was off duty for 48 hours, followed by a 12.3-hour flight duty day on the day before the occurrence, which included 7 hours of flight time. He was off duty approximately 9.5 hours before reporting for work on the morning of 22 December. He had slept well and felt rested for the flight. He had been on duty for approximately 9.5 hours when the occurrence took place.It was the first time the FO and captain had flown together.
1.5.2 Community aerodrome radio station observer/communicator
The CARS observer/communicator on duty at CYSK was hired in December 1999. Revalidation training is completed every 3 years; his last revalidation training was completed in February 2010. His next revalidation training was due in February 2013. At the time of the occurrence, the CYSK CARS was staffed as required with 1 observer/communicator.1.6 Aircraft information
1.6.1 General
The aircraft was equipped with 2 Garrett engines and 2 McCauley 4-bladed propellers. It is a pressurized aircraft first produced by Swearingen Aircraft and later by Fairchild. M7 Aerospace, a part of Elbit Systems of America, currently holds the type certificate for the SA227-AC Metro III. C-GFWX was imported to Canada in 1998. Perimeter purchased the aircraft in 2005.| Manufacturer | Fairchild Aircraft Corporation |
|---|---|
| Type and model | SA227-AC Metro III |
| Year of manufacture | 1985 |
| Serial number | AC 650 B |
| Certificate of airworthiness | 07 April 2003 |
| Certificate of registration | 19 August 2009 |
| Total airframe time | 32 982 hours |
| Engine type (number of engines) | Garrett TPE 331-11U-612G (2) |
| Maximum allowable take-off weight | 16 000 pounds |
There were no reported technical difficulties with the aircraft throughout the flight, nor any alerts or warning lights relevant to any aircraft system anomaly or failure.
1.6.2 Minimum equipment list item
The right engine single redline limit (SRL) computer was not functioning normally and had been deferred in the journey log in accordance with the minimum equipment list (MEL).Footnote 26 A placard had been installed on the instrument panel adjacent to the right exhaust gas temperature (EGT) and torque indicators. This inoperative SRL had no bearing on normal engine operation given the cold temperatures on the day of the occurrence. As per the MEL policy, the SRL item could be deferred until midnight local time on 22 December 2012 (0600 UTC on 23 December), at which time maintenance was expected to rectify the issue.The other MEL item was the left-hand essential bus lighting. The associated placard had been placed by the light switch and the appropriate logbook entries were completed. This inoperative system did not affect aircraft performance during the flight.
1.6.3 Altimeters
CARs, Standard 625, Appendix C, requires calibration of altimetry devices and air traffic control (ATC) transponders every 24 months. The captain's altimeter was last calibrated on 25 February 2011 and was installed 28 February 2011. The FO's altimeter was last calibrated on 16 August 2011 and was installed on 07 August 2012. The ATC transponder systems were calibrated on 16 December 2012.As found at the site, both altimeter barometric scales were set to 29.24 in. Hg. The left altimeter read 90 feet asl. The right altimeter indication mechanism was broken due to impact forces.
Pressure altimeters are calibrated to indicate true altitude under international standard atmosphere (ISA) conditions. Any deviation from ISA will result in an erroneous reading on the altimeter. In a case where the temperature is lower than ISA, the true altitude will be lower than the indicated altitude. The altimeter error may be significant and becomes extremely important when considering obstacle clearance in very cold temperatures. Therefore, temperature corrections for cold weather should be added to the published altitudes on instrument approach charts, but there is no regulatory requirement to do so. The Aeronautical Information Manual (AIM) states that for practical operational use, it is appropriate to apply a temperature correction when the value exceeds 20% of the associated minimum obstacle clearance.Footnote 27
The Canada Air Pilot General Pages (CAP GEN) Altitude Correction Chart shows that altimeter errors due to cold temperatures can occur at temperatures of 0°C and below. As the surface temperature was -5°C, a correction should have been made to the published procedure altitudes. A correction of 119 feet should have been added to the published sector altitude, a correction of 103 feet to the minimum published altitude for the procedure turn, and a correction of 37 feet to the MDA for the NDB Runway 27 approach, since that was the MDA used.
Since the procedure turn was executed on the opposite side of that published, and outside of the airspace to be protected, the MSA of 1600 feet asl should have been used and corrected. With the applicable cold temperature correction, the procedure turn should have been executed at 1719 feet. The MDA of 560 feet asl, when corrected, results in an indicated altitude of 597 feet. The crew had applied the required cold temperature correction only to the published MDA for the NDB Runway 27 approach and rounded it off to 600 feet asl; the circling MDA of 620 feet, which had not been obtained, was not used.
The aircraft was also equipped with a radio altimeter which indicates the height of the aircraft above ground level (agl). It is positionned on the lower left-hand corner of the instrument panel, by the captain's left knee, and is not visible to the FO. Training on the radio altimeter is included in the GPWS training and in flight training. Crews are told to set it for the “level-off” height on takeoff and then to the MDA/DH (minimum descent altitude/decision height)Footnote 28 approach minima when flying an instrument approach. Post-occurrence examination of the radio altimeter showed the setting marker (bug), set to 490 feet agl, which corresponds to 600 feet asl.
1.6.4 Terrain awareness devices
As of 04 July 2012, the CARsFootnote 29 require that aircraft manufactured on or after that date be equipped with a terrain awareness and warning system (TAWS). Aircraft manufactured before 04 July 2012 are required to be in compliance with these regulations by 04 July 2014.The occurrence aircraft had been equipped with the Sunstrand Mark VIFootnote 30 GPWS before it was purchased by Perimeter in 2005. This GPWS provides alerts and warnings for inadvertent flight into terrain. It also monitors aircraft configuration and provides warnings when the aircraft is in a non-standard landing configuration; however, it does not meet the new TAWS requirements. Perimeter was upgrading its aircraft fleet to meet the new regulations for TAWS.
One of the modes of the Mark VI GPWS is to provide advisory callouts. One of these advisory callouts is the MINIMUMS-MINIMUMS callout. As the aircraft descends through the selected height set on the radio altimeter, the MINIMUMS-MINIMUMS callout is generated. These callouts were generated during both approaches and during both circling procedures.
Another mode of this GPWS provides alerts and warnings for excessive rates of descent with respect to above ground level (agl) altitudes. This mode becomes active as the aircraft descends below 2450 feet agl. The system monitors radio altitude and rate of descent. An alert, such as SINK RATE, requires a corrective measure, while a PULL UP warning requires that the crew execute the Pull-Up In-flight Warning procedures. The chart in Figure 6 identifies the 2 envelopes of protection.
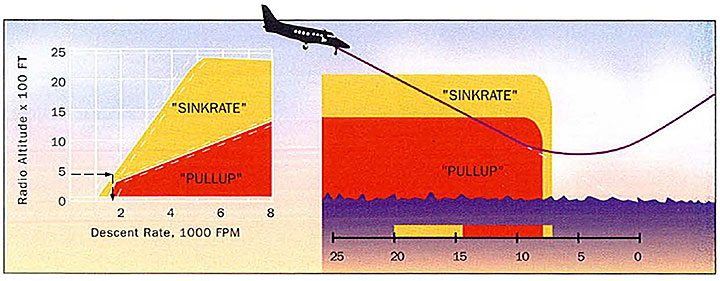
If penetrated, the inner envelope, indicated in red on the chart, activates an urgent continuous PULL UP voice message and the red GPWS warning light illuminates. When the aircraft exits the alert envelope, the voice message ceases and the red warning light extinguishes. The system may revert to the SINK RATE alert if the aircraft does not also exit that envelope during recovery.
As in the chart example, if the aircraft is descending through 2000 feet agl, a rate of descent of approximately 4400 ft/min would produce a SINK RATE alert. The same alert would only require a 1800 ft/min rate of descent to activate at 500 feet agl.
1.6.5 Global positioning system
The aircraft was equipped with a Bendix/King KLN 90B GPS. This type of GPS does not store any track data. As a consequence, no further examination of this device was performed. The KLN 90B meets the Federal Aviation Administration (FAA) TSO C129 standardFootnote 31 and is certified for en-route, terminal and non-precision instrument approach navigation. The operator had the necessary operations specification (Op Spec)Footnote 32 for the crew to conduct GPS approaches with this type of GPS unit.1.6.6 Guardian Mobility SkyTrax
The aircraft was equipped with a Guardian Mobility, Guardian 3 Globalstar flight tracking system. The on-board system sends the aircraft's GPS position to the server every 6 minutes. Information for the occurrence flight was retrieved and indicated that the unit began transmitting position reports at 1933 UTC at the start of the flight. The last position report was at 2301 UTC, approximately 5 minutes before the occurrence.1.7 Meteorological information
1.7.1 Pre-flight weather information
For pre-flight planning purposes, pilots refer to aviation routine weather reports (METAR), aerodrome forecasts (TAF), and graphic area forecasts (GFA) information. For airports where there are no TAFs, only METARs and GFAs are used. TAFs are intended to relate to weather conditions for flight operations within 5 nm of the centre of the runway. They are prepared 4 times daily with periods of coverage from 12 to 24 hours. GFAs consist of a series (6 charts) of temporally adjusted weather charts, each depicting the most probable meteorological conditions expected to occur below 24 000 feet over a given area at a specified time.For flight planning purposes, the captain had checked weather upon reporting for duty in the morning, and again at 1750 UTC.
1.7.1.1 Sanikiluaq weather prior to departure
The 1700 UTC METAR at CYSK was as follows: winds 020° True (T) at 15 knots, visibility 8 sm in light snow and drifting snow, cloud ceiling overcast at 1400 feet agl, temperature -5°C, dew point -6°C, altimeter setting 29.56 in. Hg. TAFs are not issued for CYSK.1.7.1.2 Kuujjuarapik weather prior to departure
The alternate airport for the flight was CYGW, 90 nm southeast of CYSK. The 1700 UTC METAR for CYGW was as follows: winds 010°T at 16 knots, visibility 3 sm in light snow, cloud ceiling overcast at 600 feet agl, temperature -5°C, dew point -6°C, altimeter setting 29.38 in. Hg. The TAF at CYGW, issued at 1740 UTC on 22 December 2012, valid from 1800 UTC on 22 December 2012 to 0600 UTC on 23 December 2012, indicated:Winds 010°T at 15 knots, visibility 1½ sm in light snow, cloud ceiling overcast at 800 feet agl. Temporarily from 1800 [UTC] to 2200 [UTC] visibility 3 sm in light snow, cloud ceiling overcast 1000 feet agl, 40% probability from 1800 [UTC] to 2200 [UTC] of visibility ¾ sm in light snow and blowing snow.Footnote 33 From 2200 [UTC], variable wind at 3 knots, visibility 2 sm in light snow, cloud ceiling overcast 1500 feet agl. Temporarily from 2200 [UTC] on 22 December to 0600 [UTC] on 23 December, visibility 4 sm in light snow. Remarks, next forecast at 0000 [UTC] on 23 December.METARs issued for 1700 UTC for CYSK and CYGW did not raise concerns about weather conditions for arrival after 2200 UTC. The TAF for CYGW issued at 1740 UTC allowed for CYGW to be used as an alternate.
1.7.1.3 Other weather information reviewed prior to departure
METARs and TAFs for other airports relevant to the flight were also consulted by the captain. They included Winnipeg/James Armstrong Richardson International Airport (CYWG), Manitoba; Moosonee (CYMO), Ontario; Brandon (CYBR), Manitoba;Footnote 34 Dauphin (CYDN), Manitoba; Kenora (CYQK), Ontario; La Grande Rivière (CYGL), Quebec; and Pickle Lake (CYPL), Ontario.The GFA (GFACN32) for the Prairies region, issued at 1732 UTC, valid on 23 December 2012 at 0000 UTC, was consulted for the departure and a portion of the en-route phase of the flight. The GFA (GFACN33) for the Ontario-Quebec region was consulted for the en-route and destination phases of the flight. The GFACN33, issued at 1732 UTC, valid on 23 December 2012 at 0000 UTC (Appendix E) indicated a cloud base at 3000 feet asl with tops to 22 000 feet asl, and visibility 2 to 4 sm in light snow. Scattered towering cumulus (TCU) 10 000 feet asl, bringing visibility to ¾ sm in light snow showers and blowing snow, ceilings 300 feet agl.
1.7.2 Weather obtained prior to descent for landing at Sanikiluaq
Prior to descent at 2225 UTC, the crew requested weather for CYSK from the CARS observer/communicator on the airport frequency. The following information was obtained:Observed at that time, wind 040°M at 20 gusting 25 knots, altimeter 29.25 in. Hg. The runway surface condition (RSC) was also provided. Runways 09/27, 70% loose snow, 20% trace, 10% compacted snow and ice patches. Report issued 21 December 2012 at 2133 UTC.
Later, at 2229 UTC, the crew requested weather on the Quebec FIC radio frequency. The following information was obtained:
CYSK 2200 UTC METAR: wind 010°T at 17 knots gusting 25 knots, visibility 2 sm in light snow and blowing snow, cloud ceiling overcast 1200 feet agl, temperature −5°C, dewpoint −6°C, altimeter setting 29.28 in. Hg.
CYGW 2200 UTC METAR: wind 030°T at 8 knots, visibility ½ sm in moderate snow, vertical visibility 400 feet, temperature −4°C, dewpoint −5°C, altimeter setting 29.18 in. Hg.
CYGL 2200 [UTC] METAR: wind 290°T at 10 knots gusting 17 knots, visibility 1½ sm in light snow and drifting snow, vertical visibility 1300 feet, temperature −7°C, dew point −9°C, altimeter setting 29.17 in. Hg. In remarks, visibility was noted as variable from 1 to 2 sm.
1.7.3 Environment Canada weather study
1.7.3.1 General
To assist in this investigation, the TSB requested that Environment Canada conduct a weather study for the flight from CYWG to CYSK with the alternate airport as CYGW. The weather information that follows was taken from the study provided.1.7.3.2 Area weather
The GFA for southern Hudson Bay, issued at 1732 UTC on 22 December 2012, valid at 0000 UTC on 23 December 2012, showed a strong low pressure system located over central Quebec. CYSK was located in the areas of cloud and snow covering all of southeastern Hudson Bay. Most areas west and north of the system experienced strong winds, low clouds, and low visibilities in snow and blowing snow. The snow began falling at CYGW and CYSK during the morning on the day of the occurrence, and conditions in snow and blowing snow deteriorated steadily throughout the afternoon with the approach of the low pressure system.This forecast called for prevailing visibilities between 2 and 4 sm in snow, with the exception that 25 to 50% of the area would have scattered towering cumulus cloud (TCU) giving visibilities of ¾ sm in snow showers. The cloud bases would be 3000 feet asl except in the vicinity of the TCUs, where ceilings would be as low as 300 feet agl.
There was a low-level jet stream with a wind speed peak of 40 knots from the east at 100°T between 1800 feet and 2300 feet asl. The low-level jet stream in the area of CYSK on the day of the occurrence did not reach the ground. The fact that the wind direction was constant with height indicates that directional wind shear would have been unlikely. Wind shear due to speed was possible given that the winds were so high, but the lower levels of the atmosphere were homogeneous, and the change in wind speed was mostly gradual with height, so turbulence as a result of shear would have been minimal. Mechanical turbulence between the surface and 1000 feet agl due to the high winds interacting with the ground topography would be the most likely turbulence phenomenon expected to occur with this type of atmosphere. With wind speeds less than 20 knots, the turbulence intensity would have been less than what is categorized as moderate. Moderate turbulence may have occurred with wind speeds between 20 and 30 knots.
1.7.3.3 Aerodrome forecast amendments for Kuujjuarapik
The TAF for CYGW, consulted for flight planning prior to departure from CYWG, was issued at 1740 UTC. This TAF was amended at 1936 UTC to indicate a change in the wind. The weather conditions prior to 2200 UTC were significantly changed, with a forecast ceiling of 500 to 1000 feet agl and the visibility ranging from ½ sm in moderate intensity snow to 3 sm in light snow. Wind gusts to 25 knots were also added to the forecast during this time period. From 2200 UTC, the wind was forecast to be northerly at 12 gusting to 22 knots and then become light and variable by 0000 UTC on 23 December. The forecast ceilings and visibility range from 2200 UTC to 0600 UTC remained the same as previously issued.The TAF for CYGW was amended a second time at 2211 UTC adjusting the forecast between 2200 UTC and 0000 UTC to an obscured or overcast ceiling ranging from 400 to 1000 feet agl and visibility ranging from ½ sm in moderate snow to 2 sm in light snow, with northerly winds to 8 knots. The forecast remained unchanged for the period after 0000 UTC on 23 December 2012.
The crew were not aware of these 2 TAF amendments, as the first was issued as the aircraft was taking off from CYWG and the other while the aircraft was en route. No weather forecast updates were obtained after departure from CYWG.
1.8 Aids to navigation
The navigation aid serving CYSK is the YSK NDB used for the NDB Runway 27 approach. The YSK NDB was serviceable on the day of the occurrence. GPS was also used for navigation and distance information. The crew did not report any navigation aids difficulties during the flight.1.9 Communications
There were no issues with the effectiveness of communication service with any of the air traffic services units or the CYSK CARS services involved with PAG993. The flight was on radar for departure and climb out of CYWG. It remained on radar during the cruise portion of the flight at FL230. Radar contact with PAG993 was lost as it descended below FL195 into uncontrolled airspace, approximately 54 nm from CYSK.Footnote 351.10 Aerodrome information
1.10.1 General
Sanikiluaq is a small isolated community in the Belcher Islands, Nunavut, located in Hudson Bay, approximately 780 nm east-northeast of Winnipeg. The community is served by a certified airport which is owned and operated by the Government of Nunavut, Department of Economic Development and Transportation, Nunavut Airports Division.There is 1 operational runway, 09/27, aligned 088°/268°M. The runway is 3807 feet long by 100 feet wide with a gravel surface. The Runway 27 touchdown zone elevation is 110 feet asl. The longitudinal slope from Runway 27 is down by 1.1% for the first 2300 feet, and then up 1.3% for the last 1500 feet of the runway. Crosswind conditions are expected at CYSK as runway orientation does not usually favour prevailing winds. At the time of the occurrence, CYSK was serviced by only 1 instrument approach, the NDB Runway 27 approach.
1.10.2 Runway and taxiway lighting
The runway identification lights are unidirectional flashing strobe lights situated at each end of the runway. These lights are provided at aerodromes where terrain prevents the installation of approach lights, or where unrelated non-aeronautical lights or the lack of daytime contrast reduces the effects of approach lights. At night, these lights are operated in conjunction with the runway lights. CYSK is not equipped with approach lights. To help identify the runway and align with it, the take-off and landing area boundaries of the CYSK airport are indicated by unlighted solid international orange coloured type boundary markers; these are not visible at night.The threshold and runway end lights are variable intensity red and green light units in the form of wing bars along the threshold on each side of the runway centreline. Red shows in the direction of takeoff and green shows in the direction of landing.
CYSK runway edge lights are variable intensity white lights at the runway edges along the full length of the runway, spaced at 200-foot intervals. The runway lights are operated by the aircraft radio control of aerodrome lighting (ARCAL) type K system. During the approach of flight PAG993, the runway lights were ON and set to the maximum intensity setting (B3 setting).
1.10.3 Approach slope indicator system
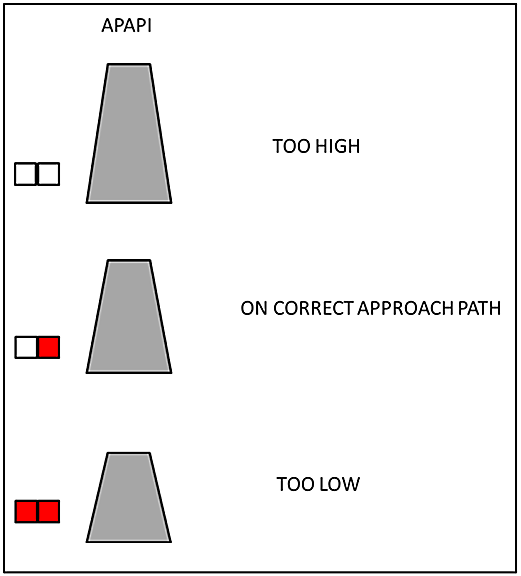
An approach slope indicator system is installed at an aerodrome to provide flight crews with visual (vertical) guidance to help in establishing a stabilized descent during an approach to landing.Both Runway 27 and Runway 09 are equipped with an abbreviated precision approach path indicator (APAPI)Footnote 36 approach slope indicator system. The APAPIs are situated on the left side of the runway, 856 feet from the threshold and consist of 2 light units in the form of a wing bar (Figure 7).
The CYSK APAPIs were verified every other day just prior to the occurrence. The APAPI units are checked for general condition, snow and ice contamination, and calibration values. The initial values found before re-levelingFootnote 37 are recorded and then the nuts on the threaded rods are adjusted until the inclinometer indicates the desired values.
There is no range of tolerance acceptable for service. A Notice to Airmen (NOTAM) is issued if the values cannot be readjusted to the specified values. The APAPI Findings/Adjustments forms for 17, 19 and 21 December 2012 showed that none of the values were out of tolerance, and therefore did not require readjustment. The last verification done on 21 December 2012 showed the system to be serviceable.
The CYSK APAPI is set for a 3-degree approach slope. The instrument approach chart depiction for the CYSK NDB Runway 27 approach, however, shows that if starting the descent at the MAP from the MDA of 560 feet asl, there is a 4.7-degree descent angle to a point approximately 20 feet above the threshold. Therefore, the initial APAPI indication seen by the crew at MDA, at the MAP would show 2 white lights indicating that the aircraft was too high. Any attempt to regain the desired 3-degree descent slope from the MAP, at 0.9 nm from the threshold of Runway 27, would initially require a greater rate of descent and likely result in a GPWS alert or warning.
1.10.4 Sanikiluaq community aerodrome radio station
At CYSK, a CARS observer/communicator completes the hourly surface weather observations and reporting. Communication equipment is used to provide operational information to flight crews. The CARS unit is housed in the airport terminal building. Normal operating hours are published in the Canada Flight Supplement (CFS), and are usually from Monday to Friday. Since the normally scheduled Keewatin Air flight on Friday, 21 December, had been rescheduled for Saturday, 22 December, and there was the additional Perimeter charter flight arriving, the CARS observer/communicator was called to work on Saturday. The METARs were available to the Perimeter crew for flight planning and arrival. The CARS observer/communicator was in communication with the flight crew and relayed runway surface conditions, wind, and altimeter setting.The visibility reported in the METAR is the prevailing visibilityFootnote 38 at the time of the weather observation. A visibility chart, depicting the distance of known objects from the airport, is used by the CARS observer/communicator to estimate the observed visibilityFootnote 39 for different horizon sectors. Flight visibility is the visibility observed by the flight crew while in flight. These visibilities may differ as they are taken from different locations and heights, and at different times. Although the CARS observer/communicator reported the visibility as 1½ sm (1.3 nm) while the aircraft was on the second approach, the crew did not acquire visual reference to the runway environment until approximately 0.7 nm from the airport, past the MAP.
1.10.5 Sanikiluaq aircraft rescue and fire fighting
The CARS observer/communicator initiated the CYSK airport emergency response plan procedures immediately after the occurrence. Prompt assistance was available by local residents, airport employees, and medical personnel who happened to be at the airport awaiting the arrival of the aircraft. There is no aircraft rescue and fire fighting (ARFF) capability located at CYSK nor was there a need for local fire fighting intervention. The Royal Canadian Mounted Police (RCMP), the law enforcement agency in place at Sanikiluaq, was notified of the occurrence and took control of the site.1.11 Flight recorders
The cockpit voice recorder (CVR) was a solid-state L3 model FA2100 with a nominal recording capacity of 2 hours. The recording included the captain and FO radio channels, cockpit area microphone (CAM) channel, an extra channel, and also 2 tracks of the last 2 hours, which included the CAM channel and a mixed radio channel (all radio channels combined). By switching the battery to OFF just prior to evacuation, the crew preserved the CVR recording, which is an important investigation tool.The aircraft was not equipped with a flight data recorder (FDR) and none was required by regulations.Footnote 40
1.12 Wreckage and impact information
The aircraft impacted rock-strewn, snow-covered terrain approximately 525 feet beyond the departure end of Runway 27, and 98 feet south of the extended runway centreline. After initial impact, the aircraft travelled 1050 feet further to the west while slewing to the right before coming to rest on an approximate heading of 60°M.All damage to the aircraft structure was due to contact with the ground. All principal structural components of the aircraft were accounted for at the site. After examination and documentation of the wreckage, it was placed in storage containers until it could be transported out of Sanikiluaq.
Various instruments,Footnote 41 including the altimeters, annunciator panel, and GPS, were recovered and sent to the TSB laboratory for examination. Due to damage, it could not be determined if the static altimeters were serviceable and properly calibrated at the time of the occurrence. The serviceability of the remaining instruments at the time of the occurrence could not be determined, nor could indication at impact be confirmed. A microscopic examination of the annunciator lights, including the lights for the landing gear position indicator, to confirm if any lights were ON at impact, was inconclusive.
1.13 Medical and pathological information
The investigation determined that there was nothing to indicate that the captain's or FO's performance was degraded by medical or pathological factors.1.14 Fire
Not applicable.1.15 Survival aspects
1.15.1 Perimeter emergency response
Perimeter's CARs Subpart 703 (Air Taxi) and Subpart 704 (Commuter) flight operations use a Type C self-dispatch system.Footnote 42 Under this system, the captain is responsible for flight watch,Footnote 43 the captain must communicate landing and departure, en-route stops, and arrival at destination. Perimeter, as the operator, must support the captain by providing a flight following system.Footnote 44 Perimeter flight following was advised of the occurrence by the captain at 2320 UTC. The company emergency response plan was put into action at that time.1.15.2 Cabin safety/aircraft occupant seats
1.15.2.1 General
The aircraft was configured with a moveable bulkhead that divided the main cabin into aft cargo and forward passenger compartments as depicted in Figure 8. Passenger seating was arranged with 5 single seats on each side of the cabin. The cargo compartment (hatched area on Figure 8), aft of the bulkhead, was loaded through a cargo door on the left side of the aircraft. Two nets were used to secure the cargo into 3 different sections.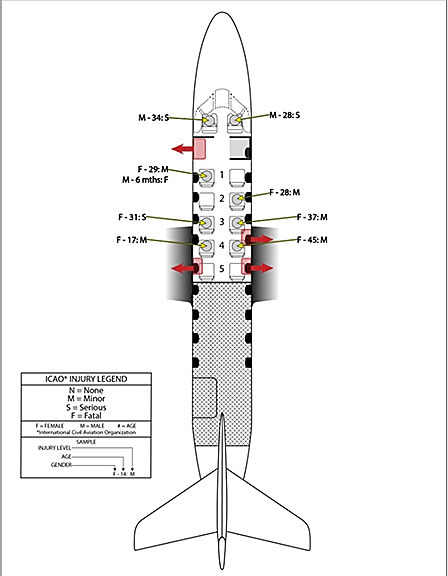
The FO's seat was completely detached, and the cockpit floor beneath the seat was destroyed. The FO received chest and face injuries.
Passengers comprised 6 adults and 1 infant. Adult passengers were all restrained by their lap belt-style safety belt. The infant was held on the mother's lap without any restraint system. Although Transport Canada (TC) recommends that infants be restrained in an approved child restraint system (CRS), it is not mandatory to do so.
Cabin seat legs and floor attachment points were broken for seats 2L, 3L, 3R, 4L and 4R.Footnote 45 All adult passengers received minor injuries except for the adult passenger seated in 3L, who received a fractured ankle. Seat support and attachment failures can subject occupants to unfavourable positions that greatly reduce tolerance to injury. When a seat does not remain securely attached to the floor, occupant injury protection offered either by the seat or by the safety belt and shoulder harness is considerably reduced.
The rear moveable bulkhead that separated the passenger cabin from the aft cargo compartment was partially detached at the floor, and cargo items, such as cans of pop, were present in the cabin.
The belly of the aircraft was compressed, and the deflection had been transmitted to the passenger cabin floor during the impact and subsequent travel across the ground. This damage also deformed the hinge structure of the forward main cabin door and placed abnormal loads on the door latching mechanism. The main cabin door, located on the left side aft of the cockpit bulkhead, was hinged on the bottom with steps and a hinged handrail incorporated into the door construction. When the cabin door is closed, the steps and handrail are immediately forward of the first seat on the left (seat 1L), where the mother and infant were seated. After impact, the orientation of the fuselage and proximity to the ground prevented the door from opening fully.
The aircraft was equipped with 3 overwing exits; 1 on the left side and 2 on the right. The forward right overwing exit was the only exit used during the evacuation. It was opened by a passenger, assisted by the FO. The FO experienced difficulty reaching the exit as the narrow aisle was blocked by the passengers, broken seats, strewn carry-on baggage and other items. The FO used the light from his personal phone to illuminate the cabin area.Footnote 46
1.15.2.2 Mother and infant
The mother holding the infant was seated in seat 1L. Because it was located directly aft of the main cabin door, this seat did not have a seat back ahead. Consequently, there was limited energy-absorbing material directly in front of the seat's occupants. The aircraft main stairway folded into the aircraft when the cabin door was closed, positioning it directly in front of their seat (Photo 2).
1.15.2.3 Briefings
Commercial Air Service Standard (CASS) 724.34(2) (b)(vii) details the individual passenger briefing pertaining to a person holding an infant:For a passenger who is responsible for another person on board, information pertinent to the needs of the other person as applicable:For Subpart 704 operations, passenger briefings are given upon boarding, prior to departure, and, upon arrival, prior to disembarking. Individual passenger briefings are completed as per the CARs and company operations manual (COM).Footnote 47 Perimeter standard operating procedures (SOP), applicable at the time of the occurrence and for 704 operations, make no mention of individual passenger briefings. Information pertinent to individual passenger briefings was not included in the training provided. The content of the COM pertaining to individual passenger briefings is not included in the training syllabus.
(A) in the case of an infant:
- (I) seat belt instructions;
- (II) method of holding infant for take-off and landing;
- (III) instructions pertaining to the use of a child restraint system;
- (IV) oxygen mask donning instructions;
- (V) recommended brace position;
- (VI) location and use of life preservers, as required.
1.15.2.4 Emergency brace position
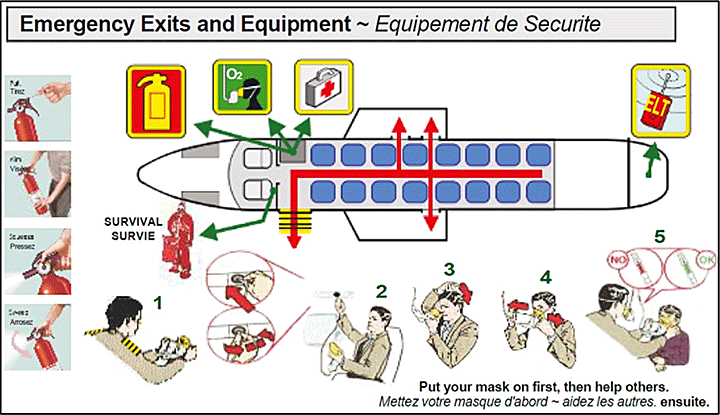
TC recommendsFootnote 48 that Canadian air operators establish emergency procedures that include brace positions. Additionally, operators are required to supply a passenger safety features card that depicts the passenger brace-for-impact position, including the brace position for an adult holding an infant.Footnote 49 The Perimeter safety features card met this requirement (Figure 9).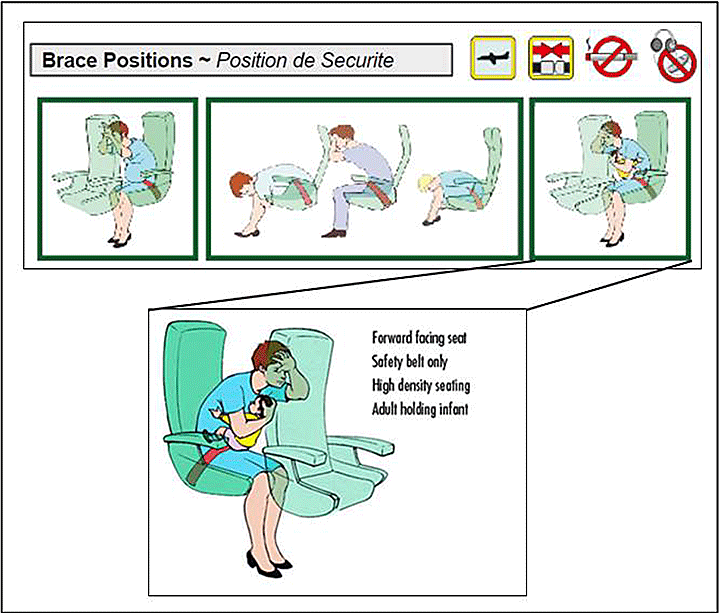
Recommended brace-for-impact positions made by the Flight Safety Foundation (FSF) in 1988Footnote 50 were based on brace positions developed by Dr. Richard Chandler of the FAA.Footnote 51 Brace information was incorporated into the TC guidance for bracing.
The recommended brace position for an adult holding an infant has the same 2 main goals as any recommended brace-for-impact position, namely
- to reduce the effect of any secondary impactFootnote 52 of the occupant's body with the interior of an aircraft, and
- to reduce flailing of body segments during a crash and the adverse effects that would otherwise result by positioning the occupant's body, or body segments, in close proximity to the aircraft surface.
Following passenger injuries in the US Airways Flight 1549 emergency ditching on the Hudson River, Weehawken, New Jersey (15 January 2009), the United States National Transportation Safety Board (NTSB) recommended (REC A-10-78) that the FAA conduct research to determine the most beneficial passenger brace position in airplanes with nonbreakover seats installed. The FAA has completed its research; results and recommendations are expected to be made public in the near future.
Biomechanical research conducted in 1979Footnote 54 found that, due to limitations in human clasping strength, it is not always possible for adults to restrain children adequately in their laps by holding onto them, and that children under 2 years old travelling in airplanes were being exposed to undue risks of injury by seating them on an adult's lap. The NTSB's 2004 analysis of the need for child restraint systems (CRS) noted that
... arm strength is not sufficient to protect even a small child. That's because commercial aircraft are designed to withstand tremendous g-forces, but humans are not. Therefore a 25-pound baby could easily weigh 3 or 4 times that amount when attempting to hold onto it during an emergency. Additionally, in crash or turbulence situations, lap-held infants were likely to contact hard structures consequently injuring them.Footnote 55Similarly, research conducted in 1992 by the United Kingdom Civil Aviation Authority (CAA) concluded that: “The carrying of infants and young children on the lap of an adult sitting on a forward-facing seat, without any recognized or approved form of restraint, is likely to promote fatalities and injuries to these children during impact situations.”Footnote 56
1.15.2.5 Emergency exits
TC Advisory Circular (AC) 700-014 defines an aircraft emergency exit seatFootnote 57 as follows:In Canada, air operators are required to ensure that aircraft seats located at emergency exits are not occupied by passengers whose presence in those seats could adversely affect the safety of passengers or crew members during an emergency evacuation.Footnote 58
- Each seat having direct access to an exit;
- Each seat in a row of seats through which passengers would have to pass to gain access to an exit, from the first seat inboard of the exit to the first aisle inboard of the exit; and
- A seat from which a passenger can proceed directly to an exit without entering an aisle or passing around an obstacle.
AC 700-014 states that a passenger's presence would be considered to adversely affect the safety of passengers and crew members during an emergency evacuation where he or she does not meet the criteria stated in the AC. Passengers seated at emergency exits must not be responsible for another person as this can hinder the opening of the emergency exit.
Although the Perimeter aircraft safety features card indicated that the main cabin door could be used as an emergency exit, for the purposes of passenger seating, Perimeter did not consider the main cabin door to be an emergency exit (Figure 10).
The COM directs that: “The PIC [pilot-in-command] shall ensure that …seats located at emergency exits may not be occupied by passengers whose presence in those seats could adversely affect the safety of passengers or crew members during an emergency evacuation.”Footnote 59
Perimeter SOPs require the FO “to keep in mind that only passengers capable of operating the emergency exits are to be seated at the exits.”Footnote 60 The issue of seating a person assisting another next to an emergency exit is not mentioned in the SOPs. In the case where passengers with limited mobility or those assisting others are present on a flight, no guidance is offered in the COM or SOPs. Although some mention as to who should be allowed to sit next to emergency exits is made in the SOPs, the practical application of these instructions in line operations had not been verified by the company or by TC.
1.15.2.6 Carry-on baggage
Carry-on baggage is defined as the personal belongings that accompany a passenger on board an aircraft. To prevent the boarding of carry-on baggage that may exceed the weight, size, shape, and total volume limitations of the approved stowage areas of the aircraft, Perimeter has a Carry-On Baggage Control ProgramFootnote 61 for screening, weighing, and determining which baggage is acceptable as carry-on baggage. Actual weights are used when calculating passenger carry-on baggage weights; however, if weight is not available, then a standard 13 pounds is used.For operations under Subpart 703 or 704, TC also requiresFootnote 62 that all carry-on baggage on board an aircraft be
- stowed in a bin, compartment, rack, or other certified location; or
- restrained so as to prevent them from shifting during movement of the aircraft on the surface and during takeoff, landing and in-flight turbulence.
The Metro III is not equipped with overhead bins to stow carry-on baggage, and the space under each seat is limited. Therefore, carry-on baggage is at times placed in the open-door closet or on empty seats, if available.
In this occurrence, most of the carry-on baggage, including coats, hats, and mittens, was placed on the empty seats. Snacks and beverages for the passengers were placed in a box on seat 1R; this box was not secured, and items were strewn throughout the cabin after the occurrence. An open-door closet partition is located directly in front of seat 1R. Passengers and crew had to step on or over the carry-on and strewn items to evacuate the aircraft. Loose items, such as personal backpacks, water bottles, and pop cans, were free to move during the crash sequence, creating a hazard for the passengers and crew.
COM, Section 10.7, Carry-On, does not stipulate how the crew are to execute or ensure that the carry-on baggage is stowed according to regulations and company procedures, given that there is limited space under the seats and there are no overhead bins in the Metro. However, crews are told to ensure that carry-on is placed under the seats, in the closet or in the cargo compartment. There is no requirement for the presence of a flight attendant for this size aircraft, and the flight crew must remain in the cockpit during the flight, except for emergency situations. Therefore, there is no way of ensuring that carry-on baggage has been re-secured prior to landing.
1.15.2.7 Child restraint systems
The Australian Civil Aviation Safety Authority (CASA) discussion paperFootnote 63 on the carriage of infants and children aboard aircraft states that: “whilst the restraint of adult occupants has steadily improved, the method of carrying infants and small children in aircraft has not really changed since the start of aviation. Consequently, the minimum standards of restraint offered to infants and small children are lower than that offered to adults.”Most jurisdictions recommend that infants and small children travel restrained in an approved CRS; however, its use is not mandatory. TC and the FAA support the use of approved CRS on commercial and general aviation flights. Nonetheless, in many countries, infants are permitted to travel on the lap of an adult. In addition, young children (2 to 12 years old)Footnote 64 may not be properly restrained while using only the seatbelt provided (Appendix F).
Operational regulations pertaining to the safe transportation of occupants using approved CRS were introduced upon publication of the Canadian Aviation Regulations (CARs) in 1996. Sections 605.26 and 605.28 of the CARs establish criteria for the use of passenger safety belts and restraint systems, and CRS. Infant and child restraint systems approved for use on aircraft in Canada and the United States are certified by Canada and US Federal Motor Vehicle Safety Standard (CMVSS 213.1 and 213, and FMVSS 213.1 and 213).
TC has indicated that several factors preclude mandating the use of appropriate CRS on board Canadian aircraft at this time. Currently approved infant/child restraint systems are designed primarily for use in an automobile. They may or may not be compatible in fit and function with aircraft seats. Therefore, in some cases, the CRS cannot be installed properly and may not perform as intended.
Not all car safety seats fit in all aircraft passenger seats. Therefore, parents have no assurance that their automobile child restraint can be used on board a particular flight. Car safety seats are not configured to be fully compatible with an aircraft seat (e.g., break-forward seat backs; no attachment point for a tether strap), nor are car safety seats fully tested with aircraft seats in mind.
TC funded an innovative research and development project to develop a prototype restraint system that would be compatible with all aircraft seats and take into account the challenges posed by the particular design and construction of aircraft seats. This project, which began in 1993, was completed in 1996 with the publication of TP 12523E, Child safety system for commercial aircraft. Results and conclusions on TP 12523E are no longer available on the TC website nor are they available at the TC library. Useful information or recommendations following this study are unknown. No similar studies or research and development are presently underway.
TC is also a member of the SAE S-9 Cabin Safety Provisions, Aerospace Standards committee that developed AS5276/l — Performance Standard for Child Restraint Systems in Transport Category Airplanes.Footnote 65 Additionally, TC is monitoring research conducted by other civil aviation authorities, such as integrated infant/child seats.
The FAA and TC recommend, but do not require, the use of CRS on commercial aircraft because they maintain that such a mandatory requirement would require parents to purchase an airline ticket for their infant, forcing some families who cannot afford the extra ticket to drive, which is a statistically more dangerous way to travel.Footnote 66 The NTSB analysed the FAA's argument and concluded that such a requirement would not result in an unreasonable burden on passengers or air carriersFootnote 67 The NTSB stated that results of laboratory data and real-world accident data demonstrated that lap-held children could not be adequately protected during a crash, and that considerable analysis of real-world air and road vehicle data found no clearly defined relationship between diversion from air travel and highway accidents or injuries.Footnote 68
At present TC does not anticipate making any changes to the regulations for the use of CRS in aircraft, nor are there any studies being conducted or education programs for operators and parents on the benefits of using CRS. Only minor changes, relevant to the content but not the direction, were made to the recent third issue of Child Restraint Systems Advisory Circular.Footnote 69 TC does anticipate that a review of the existing standards of airworthiness for CRS will be conducted in the near future; however, no date or deadline has been specified. The goal of TC's intended review will be to identify those CRS approved under United Nations standards or by a foreign government that will be deemed acceptable for use on board Canadian-registered aircraft. Following completion of the review, proposed regulatory change, if any, will be presented to the Canadian Aviation Regulation Advisory Council (CARAC) for consideration. Priorities set by TC's Standard Project Planning Application (SPPA) and a rolling 4-year work plan do not expect to table the subject of CRS for at least another 2 to 3 years.
TC does recommend the use of CRS on its website page for travel with children. No other educational programs aimed at the travelling public have been developed by TC on the recommended use of CRS. Instead TC defers to the air carriers to educate the travelling public and to promote the use of CRS. The majority of air carriers state the recommended use of CRS on their websites, but do not require their use.
See Appendix F for a discussion of policies and recommendations related to the use of CRS in other jurisdictions.
1.15.2.8 Lack of data
During its study on child occupant safety in general aviation (GA) accidents and incidents, the NTSB found that there was little information in its database on children in GA aircraft (Appendix F). Questions about how often children are involved in GA accidents, how the children are restrained, and what injuries they sustain, could not be answered due to lack of data. The NTSB noted that information on injury data is important especially if the injuries sustained by children are significantly different from those sustained by other occupants. The NTSB tracks the pilot ages for all aviation accidents in the United States, but ages for passengers are not recorded. In addition, data about the number of children who fly in GA aircraft are not available. The NTSB concluded that this type of information is needed in order to conduct research, identify risks, and outline emerging trends. Intended improvements to the NTSB aviation data management system should enable the collection of this information and evaluation of the data regarding passengers, in general, but also child passengers over the long term.Footnote 70Similarly, the TSB's database lacks information on children. There is little information pertaining to the age of passengers or injuries sustained.
In 2007, a Cessna 172L accident occurred in which the pilot and 1 passenger seated in the front right seat sustained fatal injuries; the 3-year-old child seated in the rear seat was restrained in a CRS and, although injured, survived the accident.Footnote 71 A search of the TSB database did not reveal any occurrences involving infants; this does not mean that infants have not been involved in aviation occurrences, just that the information available in the database does not reveal any occurrences involving infants.
Currently, under the Transportation Information Regulations,Footnote 72 Canadian air carriers must provide a wide range of information on their overall operations to the Minister of Transport. The number of revenue passengers and non-revenue passengers arriving, departing, and transiting, is also provided. Passenger information collected is not broken down to reflect the number of infants or children using this mode of transportation, nor is it required to be.
The passenger count on board an aircraft does not always include infants. As stated in TC Air Carrier Advisory Circular No. 0116, dated 11 April 1997:
An infant secured in a lap-held position by a parent or guardian passenger is not counted as a passenger for purposes of determining the minimum number of flight attendants required on board an aircraft, and the maximum number of occupants authorized to be on board an aircraft. An infant secured in a restraint system is counted as a passenger for purposes of determining the minimum number of flight attendants required on board an aircraft, determining the maximum number of occupants authorized to be on board an aircraft, and applying regulatory requirements such as those pertaining to oxygen, life preservers and survival equipment.Therefore, data relevant to the number of infants may be available, but not stored for easy retrieval.
Data relevant to children (under 12 years old) travelling are contained within the number of passengers and are stored in such a way that their numbers are not easily retrievable. It required some effort on the part of the air carriers questioned as part of the investigation into this occurrence, to obtain the data provided and stated in Tables 4 and 5 (Section 1.15.2.9) because, although the information may be available in their records, it is not readily retrievable from their respective databases.
Furthermore, there is no data on how many infants are travelling secured in a CRS versus those who are not. Therefore, it is not possible to confirm how many guardians have already opted to travel with a CRS. There were two recent events in the United States where guardians had chosen to purchase a separate seat for their infant in order to use a CRS. In one of the two events, it was noted that cabin crew were not familiar with the FAA rules pertaining to the use of aircraft-approved CRS. In the other event , the cabin crew, being pressed to depart on time, chose not take the time necessary for the parent to install the CRS.Footnote 73 There is a need to educate flight crews and cabin crews on CRS-related regulations and the use of CRS.
1.15.2.9 Prevalence of infant and child passengers
To determine the exposure of infants and children to commercial air travel in Canada, data were voluntarily provided by Perimeter and 3 other Canadian commercial air carriers operating in different regions of the country (operations pursuant to Subpart 703, 704, and 705 of the CARs).These companies, although different in fleet size from Perimeter, conduct operations in similar geographical areas, and service a similar passenger population. As is the case for many communities in northern Canada, Sanikiluaq is isolated. Most travel in and out of the community is by air. As part of the Belcher Islands, it is surrounded by water. Travelling by ice roads or ferry is not always an option, depending on the season.
Perimeter's passenger load data showed that a total of 160 000 passengers were flown in 2012. Of those passengers, 10 300 were children (2 to 12 years old). During the same period, there were 11 000 infants (0 to 2 years old) flown. The number of children travelling per year is approximately 6.4% of Perimeter's passenger loads. The number of infants travelling per year is equivalent to approximately 6.9% of their passenger loads. The other 3 air carriers had a combined passenger count of approximately 177 375 passengers for the year 2012, including 16 845 children (2 to 12 years old) and 8709 infants (0 to 2 years old), which represents approximately 14.4% of their passenger loads (Table 4).Footnote 74 These numbers reflect only a portion of the number of infants and children who travel by air as there are presently 583 registered commercial fixed-wing operators in Canada.
| Company | Total passengers | Total child passengers (2 to 12 years old) |
Total infant passengers (under 2 years old) |
||
|---|---|---|---|---|---|
| Number | Percent | Number | Percent | ||
|
|||||
| Perimeter Aviation | 160 000 | 10 300 | 6.4 | 11 000 | 6.9 |
| Company #2 | 2 150 | 220 | 10.2 | 144 | 6.7 |
| Company #3 | 21 009 | 1 203 | 5.7 | 854 | 4.1 |
| Company #4 | 154 216 | 15 422 | 10.0 | 7 711 | 5.0 |
| Total | 337 375 | 27 145 | 8.1 | 19 709 | 5.7 |
| Company | Total passengers | Total child passengers (2 to 12 years old) |
Total infant passengers (under 2 years old) |
||
|---|---|---|---|---|---|
| Number | Percent | Number | Percent | ||
|
|||||
| Perimeter Aviation | 1 300 000 | 85 000 | 6.5 | 90 000 | 6.9 |
| Company #2 | 115 100 | 9 000 | 7.8 | 5 100 | 4.4 |
| Company #3 | 265 395Footnote * | 12 123Footnote * | 4.6 | 11 530Footnote * | 4.3 |
| Company #4 | 1 346 046 | 134 605 | 10.0 | 67 302 | 5.0 |
| Total | 3 026 541 | 240 728 | 8.0 | 173 932 | 5.7 |
Footnotes
- Footnote *
-
The company provided data for 6 years only (2007–2012); the data in the table are those data extrapolated to 10 years.
1.16 Tests and research
1.16.1 Stabilized constant descent angle instrument approach techniques
There are 2 techniques typically used to complete the final descent on a non-precision approach (NPA): step-down descent and final descent on a stabilized constant descent angle (SCDA).The step-down descent technique involves flying an aircraft to a series of published minimum altitudes. This requires multiple changes in attitude and power to maintain a constant speed throughout the descent. This technique requires a heavier workload and more cognitive effort than the SCDA technique. Consequently, whether a crew is tired or not, they are more vulnerable to making errors inherent in the execution of the step-down descent. There is an elevated risk that the minimum altitudes that must be followed during a step-down descent will be compromised, especially if the approach is being flown manually.
A stabilized approach means a final approach flown to achieve a constant rate of descent, at an approximate 3-degree descent flight path angle, on the prescribed course to land, with stable airspeed, power setting, and attitude, and with the aircraft configured for landing.
The SCDA technique involves intercepting and maintaining an optimum descent angle to MDA, which is used as a decision altitude. The descent is therefore flown at a constant angle and constant rate of descent, requiring no aircraft configuration change. At MDA, the aircraft does not level off. Therefore, at that moment, either the required visual references are available to continue the approach and land, or a missed approach is initiated. The task simplification associated with the SCDA technique reduces the cognitive effort required for executing the approach, thereby reducing the workload and, consequently, the risk of error.Footnote 75 Additionally, the decision at which a go-around must be initiated is less subjective.
The advantages of the SCDA technique have been accepted throughout the aviation industry as being a safer way of conducting approaches. Although some Canadian operators have opted to use SCDA, several others do not, as present regulations do not require its use. TC estimates, based on informal contact with air operators and association members, that about 50% of aircraft operated under Subpart 704 of the CARs and about 20% of aircraft operated under Subpart 703 of the CARs are currently using SCDA techniques with vertical guidance as the normal procedure for an NPA. NPAs with vertical guidance, when made available for all runways, eliminate the risks associated with circling manoeuvres, and permit full realization of the safety benefits of SCDA.
Prior to the occurrence, Perimeter had not incorporated the use of the SCDA technique in its training or operations, nor was it mandatory to do so by regulations. The occurrence crew was familiar with the SCDA technique. The only reference made to similar criteria as the SCDA is within the SOPs, Section 2, Normal Operations, 2.24 Night Landings, which states, “If no glideslope guidance is available, approaches shall follow a 3-degree slope calculated by the flight crew (usually 3 miles final at 1000 feet AGL and 600-700 feet/min descent).“ The SOPs, Section 2, Normal Operations, 2.25 Landing, states, “A stable approach is essential for a safe landing so therefore the rate of descent should not be greater than 800 fpm below 1000 ‘ AGL.”
Following the TSB investigation into a controlled flight into terrain (CFIT) occurrence (TSB Aviation Report Number A09Q0203), the Board recommended that:
The Department of Transport require the use of the stabilized constant descent angle approach technique in the conduct of non-precision approaches by Canadian operators.TC has indicated that it does not intend to require operators to use the SCDA technique, but recommends its use when conducting NPAs. Since TSB Recommendation A12-02 was issued, TC has done the following in order to promote SCDA:TSB Recommendation A12-02
- Issued Advisory Circular 700-028 entitled “Vertical Path Control on Non-Precision Approaches.”
- Completed pilot examiner (PE) workshops, from coast to coast, for PEs authorized to conduct instrument rating initial and renewal flight tests, which included explanations on the new instrument approach chart depiction format being introduced by NAV CANADA.
- Revised the Aeronautical Information Manual (AIM) to address the Canada Air Pilot (CAP) approach procedures depiction changes that NAV CANADA introduced in February 2014.
- Revised the existing text in the Flight Test Guide-Pilot Proficiency Check and Aircraft Type Rating included in Exercise 15-16.
1.16.2 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:- LP 001/2013 – CVR [Cockpit Voice Recorder] Download & Transcript
- LP 011/2013 – Instruments Analysis
- LP 175/2013 – Seating Diagram Creation
- LP 070/2014 – Aircraft Performance Evaluation
- LP 086/2014 – Flight Path Diagrams
1.17 Organizational and management information
1.17.1 General
Reference in this report to company manuals, procedures and checklists, or sections thereof, refers to information within these documents which was applicable on the date of the occurrence.1.17.2 Perimeter Aviation LP
Perimeter Aviation LP is the trademark name used by Perimeter Aviation GP Inc. Perimeter Aviation LP corporate offices and its main operating base are located in Winnipeg, Manitoba. Perimeter Aviation LP also has a sub-base in Thompson, Manitoba.The organization provides both scheduled and non-scheduled air transportation services for passengers and cargo including dangerous goods. Perimeter Aviation LP has numerous certificates and operates under Subparts 703, 704, and 705 of the CARs.
Perimeter had experienced a period of rapid growth from 2005 to 2008 when 3 Dash 8s were added to the fleet. These changes required moving and training personnel from within the company and the hiring of new personnel. The company also implemented a Type B operational control system, which is considered a major change to the day-to-day Subpart 705 operations.
1.17.2.1 Dispatch/flight following
The company operates all its Subpart 705 flights (revenue, non-revenue, ferry, maintenance test, and training flights) under Type B operational control. The Type B operational control system uses co-authority dispatch and shared flight watch between the pilot-in-command (PIC) and the flight dispatcher.The COM, Chapter 6, Operational Control System – Type B (705), Section 6.3, page 6-3, provides the following interpretations:
Co-authority Dispatch - means the shared authority between the PIC [pilot in command] and the flight dispatcher in a Type B operational control system, for decisions respecting the Operational Flight Plan (OFP) prior to acceptance of the OFP by the PIC. Co-authority is in effect until brake-release of the aircraft.Operational Control – means the exercise of authority over the formulation, execution, and amendment of an Operational Flight Plan (OFP) in respect of a flight.
The role of flight dispatch in Subpart 705 operations is to exercise safe and efficient operational control over flights in conjunction with the PIC. By handling a significant portion of operational flight duties, dispatch services can significantly reduce the workload experienced by a pilot before, during and after a flight. As defined in the COM, Chapter 4, Section 4.5.4.2, dispatch activities for Subpart 705 operations at Perimeter include:
- flight planning;
- pre-flight preparations;
- monitoring maintenance issues;
- calculating fuel load requirements;
- complying with regulations;
- monitoring weather;
- updating crew on changes in weather;
- selecting routes and altitude;
- briefing flight crews; and
- flight following.
- check-in; dispatch will provide assigned aircraft, routing, scheduled loads;
- inform dispatch if they will be late for check-in;
- advise of fuel load needed;
- provide an OFP;
- report any delays due to weather or issues with aircraft; and
- report ready to depart.
The captain had worked for a number of commercial operators after leaving Perimeter in August 2008, where he flew under Type B (Subpart 705) operational control systems before returning to Perimeter in October 2012. Consequently, he had been able to rely on dispatch services assisting in flight preparations and en route for more than 4 years. As evidenced in its use for Subpart 705 operations, dispatch can play a significant role in helping to identify and manage any threats related to a flight.
1.17.3 Route and charter packages
Perimeter had developed route packages for all scheduled flights with the objective of lessening the flight crew workload during preparation of a flight. The packages include logistics information about a trip, such as crew pairing, routing, time of departure and return, number of passengers, accomodations if relevant, duty/rest time associated with the planned routing, airport facilities information, frequencies, and contact information.At the time of the occurrence, similar packages had not been developed for charter flights and, therefore, were not available to the occurrence crew. Route or charter packages are not required by regulations. Although helpful, route or charter packages, as constructed, may not necessarily assist the crew, or even dispatch, with regards to identifying any possible threats or risks associated with a particular flight or destination.
1.17.4 Flight planning
The COM, Chapter 7, Section 7.6.2, explains the division of roles between the captain and the FO in regards to pre-flight preparation. While the FO verifies the airworthiness of the aircraft, fueling, and loading of freight, flight planning takes place prior to departure and is completed by the captain. The captain must ensure that all necessary documentation and equipment is on board the aircraft, determine fuel and oil requirements, calculate the aircraft weight and balance, verify applicable NOTAMs, check the weather for departure, en route, destination and alternate airports, and complete an operational flight plan or flight itinerary. The captain must also brief the FO on such information as the weather expected en route, at destination, and the chosen alternate.The captain verified the weather on the NAV CANADA aviation weather website. The METAR for CYSK consulted at the time of flight planning showed weather was above minima for the approach. Although the instrument approach charts for CYSK were not available to the captain for flight planning, he remembered the MDA value for the approach, from having flown there before.
CAR 602.122 stipulates that any pilot operating an aircraft in IFR flight must file an IFR flight plan or flight itinerary that includes an alternate aerodrome. Weather information for the chosen alternate aerodrome must indicate that, at the expected time of arrival at the alternate aerodrome, weather will be at or above the alternate aerodrome weather minimum criteria specified in the Canada Air Pilot instrument approach charts procedures.
In order to decide on an alternate airport, the captain consulted the TAF for CYGW, the closest airport to CYSK. Using that weather information, the captain was able to determine the suitability of CYGW as an alternate airport.Footnote 76 The choice of CYGW, at the time of flight planning, was acceptable, given the forecast weather for the estimated time of arrival at CYGW (2330 UTC), if a diversion to the alternate was deemed necessary.
A pre-flight briefing between flight crew members allows them to discuss and consult on specifics affecting the flight, and assists in maintaining common situational awareness. The crew did not discuss weather conditions for the flight prior to departure.
1.17.5 Perimeter Aviation LP operational manuals
Perimeter policies, applicable to all company flight operations, are contained in the COM. The COM provides guidance for company personnel in the execution of their duties. The manual contains information required by the CARs and CASS, and is intended to supplement but not replace existing regulations. Employees are expected to be familiar with the contents of the COM, and apply the policies and procedures accordingly. Training provided by the company to its employees is expected to cover the necessary information detailed within the company manuals, procedures, and TC regulations.Aircraft type-specific information pertaining to the Metro III is contained in the applicable airplane flight manual (AFM) issued by the aircraft manufacturer, and in the company SOP manual. Pilots are required to have a working knowledge of these documents.
The COM and SOPs comply with the CASS. The COM and the flight training manual are approved by TC. With the exception of a few sections,Footnote 77 the SOPs are not subject to TC approval; however, they are subject to TC review.
SOPs and checklists provide procedural guidance to pilots for the operation of the aircraft. They assist with decision making and establishing shared mental models between flight crew members, and provide them with pre-determined solutions to various situations, whether they be associated with normal, abnormal, or emergency operations.
SOPs include division of duties and standard calls to be made by the PF and PNF; these include standard calls associated with the approach and, if necessary, the missed approach phases of flight. Checklists associated with normal and abnormal operations are in a challenge-and-response format.
1.17.6 Standard operating procedures
1.17.6.1 Standard calls
The SOPs, Section 1 Introduction, 1.6 Standard Calls and Briefings (Table 6), details the standard calls for various aircraft deviations that may occur during a flight. There are no standard calls or responses stated in the case of the GPWS sounding SINK RATE or PULL UP. There are no standard calls or reponses for conducting an NPA that involves leveling the aircraft at MDA and reaching the MAP decision point. The SOPs only contain calls for a precision approach with a decision height (DH).Table 6. Standard operating procedures (SOP) standard deviation calls (modified to eliminate calls not pertinent to this occurrence)
| Observations | Call (pilot not flying) | Response (pilot flying) |
|---|---|---|
| Any time bank angle exceeds 30 degrees | BANK | CORRECTING |
| Speed deviations +/- 10 kts | AIRSPEED PLUS DEVIATION | CORRECTING |
| Altitude deviations +/- 100 ft | ALTITUDE PLUS DEVIATION | CORRECTING |
| Heading deviations +/- 10 degrees | HEADING | CORRECTING |
| Observations | Call (pilot not flying) | Response (pilot flying) |
|---|---|---|
| Climb or descent | ALTITUDE SELECTED | LEAVING 17000 for 7000 |
| Approaching altitude | 1000 ABOVE/BELOW 200 ABOVE/BELOW |
CHECK |
| Observations | Call (pilot not flying) | Response (pilot flying) |
|---|---|---|
| Rate of climb (takeoff) | POSITIVE RATE | GEAR UP |
| Missed approach | POSITIVE RATE or NEGATIVE RATE | MAX PWR GEAR UP, FLAPS ¼ |
| Observations | Call (pilot not flying) | Response (pilot flying) |
|---|---|---|
| Below 140 kts, speeds will be called out every 5 kts of decreasing or increasing airspeed above VREF | VREF plus +/- speed deviation. (i.e. VREF plus 15, VREF plus 10) | CHECK |
| Rate of descent exceed 1000 ft/min | SINK RATE | CORRECTING |
| 1000 ft above minimums | 1000 ABOVE | CHECK NO FLAGS |
| 500 ft above minimums | 500 ABOVE | CHECK |
| 100 ft above minimums | 100 ABOVE | CHECK |
| Visual contact with runway environment | ANNOUNCES VISUAL CUES (lights–runway position) | COUNTINUING/LANDING |
| At decision height | MINIMUMS (announces visual cues) | LANDING OR |
| At decision height | NEGATIVE CONTACT | GO AROUND |
These are a few important examples (Appendix B):
- The first circling procedure (orange flight path), following the first approach to Runway 27, was conducted at 400 feet asl, 220 feet below the circling MDA. The FO called the altitude deviation. The captain executed a climb, but then descended back to 400 feet asl. The FO called the altitude again. The captain did not respond with the standard call.
- At 2255:18 UTC, following the captain's go-around call to initiate a missed approach (No. 6, yellow flight path), the standard calls for maximum power, gear up and flaps ¼ were made. However, neither crew member made the standard positive rate of climb call.
- On the climb to sector altitude of 1600 feet during the missed approach (yellow flight path nos. 6 and 7), the missed approach procedure of tracking 278° was not followed. Instead, a steady left turn was maintained during the climb. No calls or corrections were made for this deviation.
- While on the second approach to Runway 27, at 2305:05 UTC (red flight path), the FO made the standard 100 feet below minimums altitude call when the aircraft descended below the MDA of 600 feet to an altitude of 500 feet. Although the captain replied levelling, the aircraft continued down to 400 feet. The FO called 400 feet. The captain did not respond to this call but remained level at 400 feet. The FO did not question this deviation.
- At 2306:11 UTC, when the GPWS SINK RATE alert was generated, and at 2306:13 UTC, when the first of 6 PULL UP warnings were generated, neither crew member acknowledged the alerts. Neither crew member reacted to the GPWS warnings.
- At 2306:18 UTC, 1 second after the PULL UP warning ceased, while the aircraft was approximately 725 feet past the threshold, the FO indicated field conditions looked good. However, the aircraft altitude, high rate of descent, and the airspeed being too high were not raised as a concern to the captain.
- At 2306:23 UTC, when the captain called go-around, the FO prompted him with the appropriate sequence of required go-around actions as the standard calls were not forthcoming. Neither crew members made the positive rate of climb call.
1.17.7 Approaches
1.17.7.1 Approach and circling briefings
The SOPs state that the PF must conduct an approach briefing to be completed well in advance of commencing the approach, usually prior to descent.Footnote 78 This briefing should include details on- which approach will be executed;
- how the approach will be completed; and
- how the missed approach will be conducted, if deemed necessary.
In reference to briefings for circling, the SOPs, Section 2 Normal Operations, 2.23 Circling, states:
When briefing for a circling approach, the captain will determine who will be the flying pilot. Deciding factors will include:None of the abovementioned circling issues, such as rising terrain to the southwest of the airport, were considered or briefed by the crew.
The role of the flying pilot will be to fly the aircraft with visual reference to terrain and also include flight instruments in their scan.
- Geography and associated weather conditions.
- With crosswinds, turning base should be done with headwind to minimize drift, when practicable.
- Circling restrictions on approach charts
The primary role of the pilot not flying is to monitor the flight instruments. He may also assist the flying pilot in determining when to turn or descend (vectors). The pilot not flying must advise of any airspeed and altitude deviations without delay.
General procedural guidance for instrument flying in CanadaFootnote 79 states that:
There are no standard procedures to conduct a missed approach after starting visual manoeuvres. Unless the pilot is familiar with the terrain, it is recommended that:
Even with the airport in sight at circling MDA, the pilot should execute the missed approach if there is any doubt that the ceiling and visibility are adequate for manoeuvring safely to the point of touchdown.
- a climb be initiated;
- the aircraft be turned towards the centre of the airport; and
- the aircraft be established, as closely as possible, on the missed approach procedure track published for the instrument approach procedure just completed.
1.17.7.2 Night approaches
The SOPs, Section 2 Normal Operations, 2.26 Night Landing, states:Night Flying has always been, and continues to be, more dangerous than flying during the day. This is, for the most part, because of a lack of visual cues and our vulnerability as humans to be affected by illusions.
Night departures in dark conditions require full use of the aircraft flight instruments, and it is essential that the pilot achieves and maintains a positive rate-of-climb. In the absence of outside visual cues, the pilot must rely on aircraft instruments to maintain airspeed and attitude to overcome any false sensations of a climb. Night landings MUST be completed on or above glideslope guidance (ILS glideslopes, PAPI's, or VASIS's indicators) until touchdown. At no time shall a night approach be continued below glideslope guidance. If no glideslope guidance is available, approaches shall follow a 3 degree slope calculated by the flight crew (usually 3 miles final at 1000ft AGL and 600-700 ft/min descent)
1.17.8 Stable approach criteria
A stable approach involves controlling, and stabilizing several key criteria before the aircraft reaches a predefined point – usually several miles back from the airport, at 1000 feet agl. These criteria include:Footnote 80The COM does not outline the criteria for a stable approach. The SOPs, Section 2 Normal Operations, 2.25 Landing, simply states that, “A stable approach is essential for a safe landing so therefore the rate of descent should not be greater than 800 fpm below 1000 ‘ AGL.” Good stable approach policies and procedures serve as an administrative defense against possible negative outcomes, such as runway overruns and CFIT occurrences.
- Course – The aircraft is on the prescribed track to land. This avoids any excessive bank angles during the final moments before landing;
- Speed – Should be within a few nautical miles per hour of appropriate speed for approach conditions of weight and weather. This provides the slowest speed for landing, but with built in safety margin;
- Rate of descent – Should be set to maintain the glide path. This avoids excessive changes and allows an optimum closure rate to the runway surface;
- Power setting – Should be set to maintain optimum airspeed and rate of descent previously mentioned. This prevents excessive changes to airspeed and rate of descent and ensures the engines are in a power range that allows for rapid acceleration should a go-around be required; and
- Aircraft configuration – The landing gear should be down and final flap selection completed. This avoids configuration changes in the final moments of the approach which could in turn adversely affect speed, rate of descent and power setting.
Approaching the threshold of Runway 27 at approximately 180 feet agl, the aircraft was unstable in several of these parameters:
- Rate of descent – above 1800 ft/min
- Speed – VREF + 25
- Throttles – idle.
1.17.9 Discontinued approach and landings
1.17.9.1 General
In flight operations, a distinction is made between a go-around, missed approach, rejected landing, and balked landing. Transport Canada AC 700-016 (2010), Compliance with Regulations and Standards for Engine-Inoperative Obstacle Avoidance,defines the terms as follows:Go-Around -
A transition from an approach to a stabilized climb.Missed Approach -
The flight path followed by an aircraft after discontinuation of an approach procedure and initiation of a go-around. Typically a “missed approach” follows a published missed approach segment of an instrument approach procedure, or follows radar vectors to a missed approach point, return to landing, or diversion to an alternate.Rejected Landing -
A discontinued landing attempt. A rejected landing typically is initiated at low altitude but prior to touchdown. If from or following an instrument approach it typically is considered to be initiated below DA(H) [decision altitude/height] or MDA(H) [minimum descent altitude/height]. A rejected landing may be initiated in either VMC [visual meteorological conditions] or Instrument Meteorological Conditions (IMC). A rejected landing typically leads to or results in a “go-around” and if following an instrument approach, a “Missed Approach”. If related to the consideration of aircraft configuration(s) or performance it is sometimes referred to as a “Balked Landing”.Balked Landing -
A discontinued landing attempt. The term is often used in conjunction with aircraft configuration or performance assessment, as in ”Balked landing climb gradient”.Footnote 81
A low energy landing regime is defined as a condition where a rejected or balked landing is commenced after a commitment to a landing has been made. In a low-energy landing regime the aircraft is in a descent at a height of 50 feet or less above the runway, gear and flaps are in the landing configuration, thrust is stabilized in the idle range, and airspeed is decreasing. An attempt to conduct a rejected or balked landing from a low-energy landing regime may result in ground contact.Footnote 82
1.17.9.2 Company missed approach/balked landing procedure
The SOPs, Section 2 Normal Operations, 2.24 Missed Approach/Balked Landing, explains the duties and calls to be executed, but does not state the criteria or point (decision point or gate) at which to initiate a missed approach should the need arise. Criteria for initiating a missed approach at MDA or DH are stated, however, in the SOPs, Section 5 Operational Notes and Directives, 5.18 Pilot Monitored Approach (PMA). Additionally, the SOPs do not indicate that the PNF can also command a go-around. From a crew resource management (CRM) perspective, the ability of either pilot (PF or PNF) to command a go-around is fundamental to reducing approach-and-landing accidents (ALA).The SOPs stipulate the steps and standard calls shown in Table 7 when executing a missed approach:
| Pilot flying duties | Pilot not flying duties |
|---|---|
| Calls “GO AROUND” | Acknowledge “Check Go Around” |
| Calls “Max Power, Gear up, flaps ¼ Selects go around on flight director and rotates aircraft at a rate of 2 degrees per second to match flight director or rotates to 10 degrees nose up attitude simultaneously advancing the power levers to max power | Taps PF hands and sets power to briefed power setting and selects gear up and flaps up Calls “Max Power Set” and States V2 speed |
Either Pilot Observes and Calls “POSITIVE RATE”
|
|
| Confirms and Calls “Three Positive Rates of Climb” |
Calls Level Off |
| Accelerates to VYSE and Calls “FLAPS UP” |
Retracts Flaps |
| States “I have the Powers” | States “You have the Powers” |
Following the captain's go-around call, power was set to maximum, gear was retracted, and the flaps set to ¼ position. The positive rate of climb calls were not made by either pilot. Flaps were not brought to the full-up position as the aircraft impacted the ground before this item could be executed (Appendix G).
The balked landing climb performance for the SA227-AC (Metro III) published in the AFM uses the gear-down and full-flaps configuration to provide climb data at specified climb speeds. These data are based on the balked landing procedure below (Figure 11).
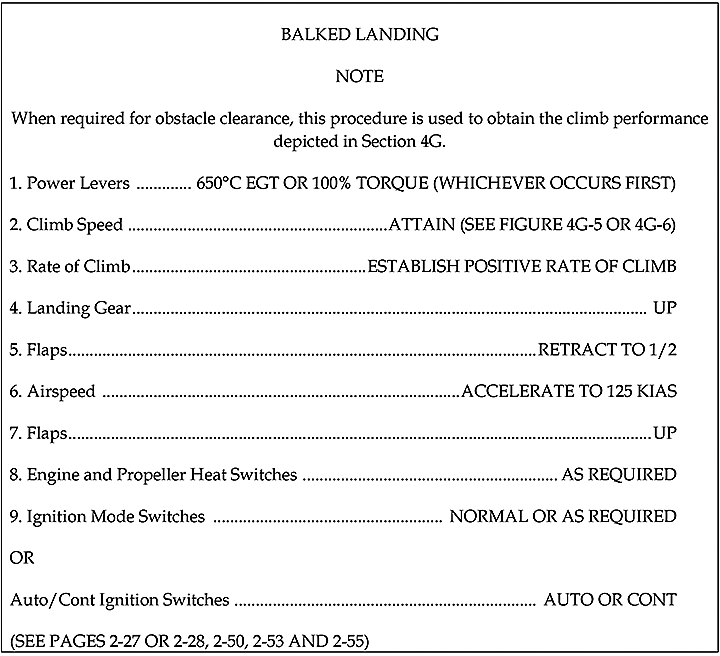
The company tested the AFM procedure in a controlled environment in the late 1990s, early 2000s. Testing was done in a Metro II aircraft, as Perimeter did not acquire a Metro III until 2005. Although the company SOPs do not distinguish between high-energy and low-energy states, training includes go-arounds from low-energy states. The AFM for the Metro II suggested an initial climb speed of 96 knots, which was considered by the company as very slow for a Metro II with the gear and flaps deployed. The company also felt that on a hot day with a fully loaded aircraft, a positive rate of climb in the landing configuration would not be possible. The company felt the best procedure to ensure the aircraft was climbing away from the ground was to emphasize the pitch-up and immediate configuration change. In 2005 when Perimeter acquired a Metro III, most of the Metro II procedures, culture, and philosophy carried over to the Metro III.
Crews were trained to wait for the positive rate of climb call to reconfigure the aircraft after a go-around mainly when windshear was encountered. This was not necessarily the case for balked landings and go-arounds in other situations. However, for the previous 3 years the company had been training pilots to wait for a positive rate of climb before requesting the configuration change. Although this change was not reflected in the SOPs or training at the time, training now emphasizes the need to confirm a positive rate of climb, in any go-around situation, before requesting any configuration change. In the fall 2013, the company initiated work to incorporate this change in the SOPs.
1.7.9.3 Balked landing climb performance
The aircraft trajectory and performance were calculated based on the following information:- the CVR;
- Skytrax GPS positions;
- GPWS alerts;
- airport information;
- the AFM;
- observation of the passing aircraft over the runway
- meteorological data at the time of the occurrence.
The weather conditions in which the aircraft was operating were conducive to icing, and both the CVR and wreckage indicate the presence of a thin line of ice accumulation on the leading edge of the wings. This accumulation was considered negligible by the crew. The AFMFootnote 84 provides the balked landing performance for the aircraft being encumbered by ice accretions, to the extent tested during aircraft certification. According to the AFM, chart 4H-7, the expected rate of climb would be 1280 ft/min, at a speed of 122 knots indicated airspeed (KIAS) when using the following occurrence conditions:
- temperature of −5°C
- pressure altitude of 800 feet
- engine anti-ice ON
- encumbered by ice accumulation
- calculated aircraft weight of 14 200 pounds.
1.17.10 Ground proximity warning system training
As specified in the company flight training manual, GPWS awareness training is covered in the 1-hour CFIT training module, and in the Metro flight training as part of the systems management portion of the flight training.Chapter 8 of the COM, Section 8.9.6, states that, in the event of a GPWS warning, “[…] pilots should immediately, and without hesitating to evaluate the warning, execute the appropriate pull-up action.” It also specifies that, “This immediate pull-up procedure should be followed except in clear daylight visual meteorological conditions when the flight crew can immediately and unequivocally confirm a false GPWS warning.” The content of the COM pertinent to GPWS is not reviewed in training; however, crew reaction to warnings is reviewed during the annual CFIT training.
The SOPs for the SA227 do not provide direction on necessary actions to take in the event of a GPWS warning or alert. There are no standard calls or responses stated in the case of the GPWS generating SINK RATE or PULL UP warnings.
The AFM contains a supplement for the GPWS that comprises the same information in regards to the operation of the system as in the Mark VI Warning System Pilot's Guide. The guide lists the recommended procedures to be followed after an in-flight activation of the alerts or warnings. Information pertaining to the parameters that cause activation of the different GPWS warning was covered in Section 1.6.4 of this report.
For in-flight activation of the SINK RATE alerts, page 29 of the guide recommends to level the wings and reduce the rate of descent until the visual and aural alerts stop. For in-flight activation of the PULL UP warning, page 28 of the guide recommends:
If the aircraft is in instrument meteorological conditions (IMC) or at night when the warnings or alerts are activated:The investigation concluded that current company pilots' knowledge on the aircraft parameters that will trigger GPWS alerts and warnings is limited. However, crew do know that if the runway is visual and a warning or alert is received, they should first acknowledge the warning or alert and then state their intent to continue the approach or not.
- Level the wings and simultaneously pitch up at a rotation rate of 2 to 3 degrees per second to the best angle of climb attitude.
- Apply maximum power.
- Monitor radio altimeter for trend toward terrain contact and adjust pitch attitude accordingly upward as necessary, honoring pre-stall buffet warning.
- Continue maximum climb straight ahead until visual and aural warnings cease.
- Advise air traffic control as necessary.
1.17.11 Safety management systems
The following information regarding safety management systems (SMS) is taken in part from International Civil Aviation Organization (ICAO), Document 9859, Safety Management Manual, Chapter 5. The principles of SMS expect operators to proactively manage their safety risks and to have the necessary systems in place to ensure their operations comply with regulatory requirements on an ongoing basis. The system is designed to improve safety continuously by identifying hazards, collecting and analysing data in order to continuously assess safety risks. SMS seeks to proactively contain or mitigate risks before they result in aviation accidents and incidents.SMS integrates operations and technical systems with the management of financial and human resources to ensure aviation safety or the safety of the public. Having an SMS in place implies constant measurement, evaluation, and feedback into the system in order to be proactive about safety.
With the help of SMS reporting, many operators are collecting, analysing, and using their own safety data relevant to the different phases of flight to target specific areas of an operation that pose the greatest risk. Flight operational quality assurance (FOQA)Footnote 85 is one example of data collection and analysis with the purpose of advancing safety within a company.
ICAO mandated its 190 member states, including Canada, to develop and implement SMS to achieve an acceptable level of safety in aviation operations. Transport Canada committed to the implementation of SMS in aviation organizations in 2005. Canadian operators functioning under Subpart 705 of the CARs were given until 2010 to implement SMS.
Perimeter's SMS was finalized and accepted by TC in May 2010. The company's SMS manual describes the policies and procedures directing SMS activities within its operations. Although Perimeter developed an SMS to comply with the requirements for the implementation of SMS for Subpart 705 operations, the company applies SMS to all its operations, including Subpart 703 and 704 operations.
An integral component of an SMS is a non-punitive reporting system. With a non-punitive reporting system, employees of an organization are given qualified immunity from punitive actions to encourage them to report any safety-related events or concerns. SMS reporting is considered as a positive approach to safety and is encouraged.
While management response to issues raised through Perimeter's SMS reporting system was generally considered adequate by staff, one ongoing concern raised relates to the issue of extensions to flight crew duty day. CAR 700.16 allows for an extension of the flight crew duty day for unforeseen circumstances. Perimeter had recently expanded the description and clarified the meaning of “unforeseen circumstances” in the COM to assist crews in determining if these conditions were applicable. The parameters that define “unforeseen operational circumstances” are contained in the CARs and in Perimeter's pilot contract.
Also, extension of the duty day can be planned by changing a flight designated as a Subpart 704 operation on the outgoing trip to a Subpart 703 operation on the return trip. Extension of a duty day in this manner is apparently common practice within the company. This practice is also common to many other operators, as current TC regulations allow operators to do so. Pilots at Perimeter, including the occurrence captain, had reported this safety concern through the SMS reporting system, but at the time of the occurrence, flight crews did not consider that it had been adequately addressed.
1.17.12 Safety case
Perimeter's SMS manual defines a safety case as:A risk assessment exercise completed by the operations group to ensure that certain existant risks are assessed, addressed and mitigated as much as possible before deployment. Safety case studies are used as a proactive means to anticipate, prepare for, and mitigate potential and possible latent hazards caused by corporate or regulatory change. Safety cases shall, whenever possible, employ a team approach involving front-line employees and managers with the SMS Manager providing facilitation. A safety case study shall be completed during any of the following changes:CYSK is similar to many other airports at which Perimeter operates on a daily basis. The number of Perimeter flights into CYSK had increased from January 2012 to December 2012; initially starting with just a few flights per month going up to 11 flights per month for both November and December 2012, for a total of 62 flights in 2012. As a result, CYSK was not considered a new destination when the 22 December 2012 charter request was made. Therefore, management did not consider it necessary to conduct a safety case for that destination.
The above list is not necessarily exhaustive and therefore a safety case may be initiated at any time that a manager thinks it is appropriate. If the risks remain assessed as too high, then the flight(s) would normally be cancelled.
- prior to significant changes in operations or maintenance systems, processes or procedures;
- as soon as possible in changes in key personnel;
- prior to new routes or a change to the existing route structures;
- prior to the introduction of a new type of aircraft into the fleet;
- prior to new or substantially different avionics systems being introduced;
- prior to new destination areas and/or airports; and,
- prior to, or as soon as possible to, major changes in requirement in applicable regulations.
TC had not required that a safety case be completed for other CYSK charter flights prior to this occurrence. The possible risk factors associated with flights conducted to CYSK, whether by day or by night, had not previously been identified by TC or Perimeter.
1.17.23 Transport Canada oversight
The objective of Transport Canada Civil Aviation's (TCCA) surveillance programFootnote 86 is to confirm that the holder of a Canadian Aviation Document (CAD) complies with the CARs. Where a CAD holder maintains more than one certificate (approved maintenance organization, Air Operator's Certificate, airport certificate, etc.), TCCA takes an enterprise approach to surveillance. That is, all certificates held by the enterprise are subject to the same surveillance activity. TCCA expects that the enterprise complies with all the required areas of the CARs, including SMS.TCCA's surveillance program comprised 3 main surveillance activities: SMS assessments, program validation inspections (PVI);Footnote 87 and process inspections (PI).Footnote 88 SMS assessments and PVIs are system surveillance activities whereas PIs are a process surveillance activity.
The company's SMS is assessed, as well as the company's ability to maintain effective compliance with all regulatory requirements. The CARs, Part I - General Provisions, CAR 107.03, states that an SMS shall include:
TC's Staff Instructions, SI SUR-001, Issue No. 4, explains that:
- a safety policy on which the system is based;
- a process for setting goals for the improvement of aviation safety and for measuring the attainment of those goals;
- a process for identifying hazards to aviation safety and for evaluating and managing the associated risks;
- a process for ensuring that personnel are trained and competent to perform their duties;
- a process for the internal reporting and analyzing of hazards, incidents and accidents and for taking corrective actions to prevent their recurrence;
- a document containing all safety management system processes and a process for making personnel aware of their responsibilities with respect to them;
- a quality assurance program;
- a process for conducting periodic reviews or audits of the safety management system and reviews or audits, for cause, of the safety management system; and
- any additional requirements for the safety management system that are prescribed under these Regulations.
A Program Validation Inspection (PVI) is intended to provide a review of sufficient depth to determine the level of compliance and effectiveness of a component. The use of a PVI will provide sufficient assurance that the certificate holder has employed effective policies, processes and procedures to meet regulatory requirements.A PVI is a smaller, more focused surveillance activity directed at a component, for example, a quality assurance program. If the inspection has identified findings of non-compliance then the company must submit a corrective action plan to rectify items defined in the findings within a certain timeframe. The corrective action plan may be short term or long term. Follow-up inspections are completed to ensure ongoing compliance with regulatory requirements and that the approved corrective action plan has been implemented.
A PVI differs from an assessment in that it does not look at the entire SMS. It is used to determine that all the requirements of a particular component of the SMS model or other parts of the regulations are documented, implemented, in use and effective. PVI will be used as the routine surveillance method in place of traditional inspections.Footnote 89
A PI examines a single process to determine if it meets regulatory requirements. It is intended to provide information to support decisions related to the level of risk associated with a certificate holder and what additional surveillance may be required. A PI will be conducted to follow up on observations from a previous PI or on items that have been specifically identified as being possible hazards, after changes to a particular division of the operation. A PI shall only be conducted for cause. For example, following an occurrence, or when there is growth or change within a company, a PI will be conducted on an as-needed basis.
TC conducts these surveillance activities to ensure that the policies and proceduresFootnote 90 put in place and written in the company manuals such as the SMS, COM and SOPs, are in fact put into practice.Footnote 91 The objective is to ensure that a company's operations are conducted in compliance with the regulations, but also to ensure that the company's operations are run safely. The identification of any possible hazardsFootnote 92 is also part of the surveillance activities. Risk assessments are conducted for any hazards that may be identified. Findings resulting from a surveillance activity identify areas that are not compliant with regulatory requirements. If a procedure or practice does not go beyond the confines of the regulatory requirements, then it will not necessarily result in a finding.
TC conducted an annual PVI for Perimeter, from 10 to 14 September 2012, for the purpose of verifying if Perimeter had an effective quality assurance program (QAP) and safety oversight system. The PVI identified 6 findings in the following areas:
- Documentation/records management: noted were certain sections in the COM that were out of date or incomplete.
- Safety oversight/risk management (2 findings): noted was that the SMS manual did not contain timelines for long-term corrective action plans.
- Training/training, awareness and competency: noted for Subpart 705 operations; flight attendant records did not contain information pertaining to flight deck admission control training or certain information relevant to dangerous goods training.
- Quality Assurance Program (2 findings): noted were missing or omitted details relevant to the QAP applicable to the maintenance program inspections timelines and manual.
- Perimeter submitted its corrective action plan and it was approved by TC on 10 December 2012. Regular discussions and an exchange of emails took place between the company and TC to keep abreast of expectations and corrective action plan timelines for the different items to be addressed.
As a result of this occurrence, TC called for a “post-occurrence PI”, which was conducted at the end of January 2013. This PI, based on preliminary information on factors that could possibly have contributed to the occurrence, was conducted solely to evaluate the process used by Perimeter for oversight of its charter operations. The January 2013 PI made 2 observations:
- Non-compliance with Perimeter's own policy on conducting safety cases
- A gap in Perimeter's Cabin Safety training program documentation with respect to missing key regulatory requirements (i.e., written procedures for briefings existed; however, there was a lack of training with regards to the required safety briefing, exit seating/briefing, individual passenger briefing).
The hazard of not restraining the infant was not identified. Given that the use of CRS is not required by current regulations, there was no non-conformity to regulatory requirements.
1.18 Additional information
1.18.1 Human performance issues
A number of factors, such as frustration, fatigue and stress, can influence human performance in carrying out safety-critical activities. These factors can result in the following behaviours:- irritability,
- willingness to take risks,
- normal checks or procedures ignored,
- inappropriate corrective action (problem-solving abilities),
- mis-interpretation of the situation, and
- poor judgement of distance, speed, and/or time.
1.18.1.1 Frustration
Frustration is defined as the feeling of anger or annoyance caused by being unable to do something.Footnote 94 Time pressure increases the likelihood of risky decision making, with less time spent accessing information when one is under time pressure compared to when under no time pressure.Footnote 95 As well, time pressure amplifies frustration or anger that is associated with delay, and results in the frustration or anger persisting across multiple situations even once the delay-causing agent has been removed. Frustration or anger can lead to one underestimating the likelihood of risky events occurring, and to choosing a more risky option than would be chosen in the absence of frustration or anger.Footnote 96People most commonly use swear words to express anger or frustration.Footnote 97 Estimated average spoken word rates of swearing range from 0.5 to 0.7%, or between 80 and 90 swear words per day (5.3 per hour).Footnote 98 The captain used 43 expletives in conversation with the FO during the 2-hour period preceding the occurrence, a rate of approximately 21.5 swear words per hour. This type of behaviour was seen as being out of character for the captain.
1.18.1.2 Fatigue
Fatigue was examined to verify if it may have affected the crew's ability to perform their duties. Analysis of their 72-hour work/rest history did not point to fatigue as a performance-altering factor. Neither crew member felt that fatigue was an issue before the flight.However, both crew members had expressed feeling tired during the flight as it had been a long day. Additionally, the occurrence took place towards the end of the afternoon circadian dip, when feelings of fatigue are more pronounced and can affect performance.Footnote 99
Although he had been in bed for 8 hours the night before the occurrence flight, the captain had 6.5 hours of sleep, considering the 1.5-hour wake period he experienced during the night. Based on the captain's 1.5-hour wake period and resultant shortened sleep duration the night before the flight, acute sleep disruptionFootnote 100 may have played a role in the captain's behaviour during the flight by increasing the risk for fatigue and its associated performance decrements. Furthermore, circadian rhythm timing may have exacerbated the fatigue brought on by the acute sleep disruption. The FO had approximately 8 hours of sleep the night before the occurrence flight. As he had not experienced sleep disruption during the night, fatigue was considered less of a risk factor for the FO. At the time of the occurrence, both crew members had been awake for approximately 11 hours.
1.18.1.3 Stress and performance
Increased stress levels can adversely impact a pilot's ability to perceive and evaluate cues from the environment, and may result in attentional narrowing. Studies have shown that individuals under stress tend to limit their attention to stimuli they perceive to be most important or most relevant to the task at hand.Footnote 101 This may result in pilots only paying attention to certain cues while excluding others, which in turn leads to a loss of situational awareness. It is crucial that pilots continually re-evaluate the situation in which they find themselves in order to determine whether they accurately perceive it, and if the plan is working out as expected, or if a change in the plan is required.1.18.2 Crew resource management
1.18.2.1 General
For each and every flight, pilots must successfully interact with each other, their aircraft, associated checklists, manuals, and their environment to effectively manage threats, errors, or undesired aircraft states that may be encountered. The objective of CRM is to reduce human error in aviation by ensuring better crew coordination. CRM is widely accepted as the use of all resources available to the flight crew to ensure safe and efficient flight operations.One skill associated with good CRM is effective crew communication. With good communication comes good decision making, workload management, problem solving, and better situational awareness. Crew members must have a common mental model of the current aircraft state and environmental information, which will lead to better anticipation and coordination of their actions towards a common goal.
1.18.2.2 Crew resource management training
Appropriate, representative CRM training has been shown to improve attitudes towards crew coordination and to allow for more effective team work. It has also been shown to improve flight crew performance and the ability to cope with non-routine situations.Footnote 102 Research has also shown that recurrent training is necessary to maintain the concepts learned during CRM training. If these concepts and, consequently, the positive effects of CRM training are not reinforced, they tend to disappear.Following a TSB investigation into a runway excursion in British Columbia in July 1993 (TSB Aviation Investigation Report A93P0131), the TSB recommended (A95-11) that TC establish guidelines for CRM and decision-making training for all operators and aircrew involved in commercial aviation. TC's response to the recommendation addressed only Subpart 705 operationsFootnote 103 and did not require CRM training for Subpart 703 and 704 operations.
Following a CFIT accident in Saskatchewan in January 2007 (TSB Aviation Investigation Report A07C0001), the TSB recommended (A09-02) that TC require commercial air operators to provide contemporary CRM training for Subpart 703 and Subpart 704 pilots.
Since its initial response to Recommendation A09-02 in 2010, TC has worked on developing a contemporary CRM training standard to replace the existing standard, which does not reflect modern CRM training concepts. TC intends to extend this training to Subpart 702, 703, and 704 operations, and would include threat and error management (TEM) as the most recent and widely accepted approach for CRM training.
The TSB investigation into a Boeing 737-210C CFIT occurrence in Resolute Bay, Nunavut, in August 2011 (TSB Aviation Investigation Report A11H0002), again addressed the need for better up-to-date regulatory action, training, and guidance in regards to CRM. The report explains how CRM training has evolved since its introduction in the late 1970s, and how the TEM model recognizes the importance of undesired aircraft state management as it represents the last opportunity for flight crews to prevent an adverse outcome.Footnote 104 As a consequence, the TSB issued a Safety Concern in its final report on that accident, stating that, without a comprehensive and integrated approach to CRM by TC and aviation operators, flight crews may not routinely practise effective CRM.
Initial research has supported links between TEM and CRM and has shown that:
TC has initiated measures to change the CRM training standard. A focus group consisting of TC and industry representatives met in January 2012 and submitted a final report in February 2012. The focus group report proposed components of a contemporary CRM training standard for CARs Part VII commercial operators, but recommended against a set time for CRM course duration and any formal accreditation for CRM instructors. The Civil Aviation Regulatory Committee (CARC) accepted the TC focus group recommendations, and on 24 April 2012 directed that a contemporary CRM training regulations and standard be developed for CARs Subpart 702, 703, 704, and 705 operations.
- crews who develop contingency management plans, such as proactively discussing strategies for anticipated threats, tend to have fewer mismanaged threats;
- crews who exhibit good monitoring and cross-checking usually commit fewer errors and have fewer mismanaged errors; and
- crews who exhibit strong leadership, inquiry, and workload management are typically observed to have fewer mismanaged errors and undesired aircraft states than other crews.Footnote 105
It is not yet known how detailed TC's new training standard and guidance material will be compared to the existing standard, or when the new standard will come into effect. Nor is it known how TC will monitor if operators apply the new training standard to ensure that flight crews acquire and maintain effective CRM skills.
As of January 2015, TC, in its review of Recommendation A09-02, agrees with the intent of the recommendation.
TC continues to work on the development of standards and guidance material for CRM and updated pilot decision making (PDM) to be incorporated in the CRM modules. Public consultation on proposed amendments to the standards is underway, and the standards are expected to come into effect in late 2015.
The Board is encouraged that action on this recommendation is nearing completion. The proposed course of action should substantially reduce or eliminate the safety deficiency identified in Recommendation A09-02. Until the standards are amended and fully implemented, this safety deficiency will continue to exist. In its annual review of responses to its recommendations in 2015, the Board considered that TC's response on this issue indicates Satisfactory Intent.Footnote 106
Although not mandatory for Subpart 703 and 704 operations, Perimeter recognizes the benefits of CRM training and provides it to its flight crews. CRM training is given during the annual ground school training and the content is approved by TC. Information collected for this investigation indicated that crews were somewhat bored with the recurrent CRM training, and did not find it to be a productive exercise as the same examples and subjects were reviewed every year.
The occurrence captain had received CRM training while employed with his previous employer for Subpart 705 operations, and was expected to receive CRM training with Perimeter within a year. The FO had received Perimeter's CRM training in 2011. Although they had not worked together before, both the captain and the FO felt that they had a good rapport and did not perceive any CRM or communication difficulties throughout the flight.
1.18.2.3 Crew communication
In order to align crew situational awareness and optimize the decision-making process, crew members must be effective communicators and must feel comfortable in providing input to each other. This can be a challenge in the cockpit when faced with time pressures, competing priorities, or an inappropriately balanced trans-cockpit authority gradient. Trans-cockpit authority gradient refers to the manner in which the captain and the FO interact. If a steep trans-cockpit authority gradient exists, either due to experience levels or personality types, there is an increased risk that decisions will be made based on incomplete or inaccurate information.Footnote 107It is important for a captain to recognize that, in most cases, inexperienced FOs will be predisposed to use subtle, non-aggressive communication strategies to voice concerns that they are afraid to raise for fear of being wrong, or of being chastised for questioning a more experienced individual.
Practising assertiveness techniques can enhance CRM training. It is important because it trains less senior team members to feel comfortable providing input to a more senior team member, and to communicate this information in an effective way. It also trains senior team members to accept input without feeling threatened.Footnote 108
1.18.2.4 Threat and error management
In order to understand the chain of events that led to this occurrence, the investigation used the TEM model. The following information on the TEM model and associated table are taken from papers written on the subject.Footnote 109,Footnote 110TEM is defined as the analysis of potential hazards and the taking of appropriate steps to avoid, trap, or mitigate threats and errors before they lead to an undesired aircraft state. The key principles behind TEM are anticipation, recognition, and recovery.
When applying TEM to analyse the relationship between safety and human performance in a context such as flying, it is important to keep the user's perspective in mind. The user can be the flight crew, management, senior management, flight operations, maintenance, or air traffic control.
For flight crews, threats are defined as events or errors that occur beyond the influence of the flight crew. They increase operational complexity and must be managed to maintain a certain level of safety. During typical flight operations, flight crews need to manage various and, at times complex, events. For example, events could include dealing with adverse meteorological conditions, aircraft malfunctions, and errors committed by other people outside of the cockpit, such as air traffic controllers or maintenance workers. These events can be viewed as threats because they have the potential to negatively affect flight operations by reducing safety margins.
The TEM model groups threats under 2 basic categories: environmental threats and organizational threats.
Some environmental threats can be planned for and some will occur unexpectedly, but they all have to be managed by flight crews in real time. Organizational threats, on the other hand, can be controlled by the operator and are usually latent in nature. Although flight crews remain the last line of defense, there are usually earlier opportunities for the operator to mitigate organizational threats. Examples of environmental and organizational threats appear in Table 8.
| Environmental threats | Organizational threats |
|---|---|
|
|
Footnotes
- Footnote *
-
List not inclusive
The effect an error will have on safety depends on whether the flight crew detects and responds to the error before it leads to an undesired aircraft state and to a potential unsafe outcome; an error that is not detected cannot be managed. An error that is detected and effectively managed has no adverse impact on the flight. Examples of errors would include the inability to maintain stabilized approach parameters and failing to give a required callout.
TEM divides flight crew errors into 3 types:
- aircraft handling
- procedural
- communication
An undesired aircraft state may include flight crew-induced aircraft position or speed deviations, misapplication of flight controls or incorrect systems configuration, all of which are associated with a reduction in margins of safety. As with errors, undesired aircraft states can be managed effectively, returning the aircraft to safe flight. If mismanaged, they can lead to an additional error, undesired aircraft state, or worse, an incident or accident.
The use of the TEM model assists in educating, not only flight crews, but all those involved in flight operations, on the anticipation, recognition, and recovery from existing threats and errors.
Based on information on threats and errors collected in the Line Operations Safety Audits (LOSA)Footnote 112 Archive, the following statistics are of interest:
Threats:Essentially, from the pre-flight preparation to engine shutdown after landing, flight crews are constantly working on threat, error, and undesired aircraft state management. If threats and errors are not detected and managed throughout the whole flight, the probability of adverse consequences increases.
Errors:
- The typical flight (regularly scheduled, normal operations) encounters an average of 4.2 threats per flight; 3 are likely to be environmental threats and 1 is likely to be an organizational threat. Seventeen percent of flights encounter 7 or more threats per flight. Therefore, multiple threats are the standard and need to be managed.
- About 40% of all threats occur during the predeparture/taxi-out phases of the flight and 30% occur during descent/approach/land phases. For environmental threats, the busiest phase of flight is descent/approach/land, while for organizational threats, the busiest phase is predeparture/taxi-out.
- Most threats are successfully managed (85-95%). The average across the LOSA Archive is 90%. Therefore about one tenth of all threats are mismanaged by crews.
Undesired aircraft state:
- 80% of flights have 1 or more errors, with an average of approximately 3 per flight.
- 20% of flights have no observable errors.
- 40% of all observed errors occur during the descent/approach/land phases of flight. 30% of errors occur during predeparture/taxi-out when crews are preparing the flight.
- Procedural errors make up half of all errors, but less than one-quarter of mismanaged errors.
- Three-quarters of all mismanaged errors are aircraft handling errors with communication errors comprising the remaining few percent.
- Checklist errors are the most common procedural error, followed closely by callout and SOP cross-verification errors. Briefing errors are less common.
- About 25% of all errors are mismanaged. 6% of all errors lead to additional error and 19% result directly in an undesired aircraft state.
- 36% of all mismanaged errors are manual handling/flight control errors. 16% of mismanaged errors are automation and system/instrument/radio errors,
- 5% are checklist errors and 3% are crew–ATC communication errors.
- About 30% of all undesired aircraft states occur as part of a chain of events that starts with a threat that is not managed well and leads to a crew error, which in turn is mismanaged, leading to an undesired aircraft state.
1.18.3 Instrument approach design
1.18.3.1 General
Instrument approach procedures in Canada are developed based on a TC manual entitled Criteria for the Development of Instrument Procedures (TP308/GPH209). According to TP308, “obstacle clearance is the primary safety consideration in the development of instrument procedures.”TP308 states that the optimum descent path for a non-precision final approach segment is 318 feet per nautical mile, or an angle of 3 degrees, and its use is recommended.
In the case of the CYSK NDB Runway 27 approach, the NDB is the MAP and is located 0.9 nm from the threshold of Runway 27 (Figure 12). Using a threshold crossing height of 40 feet, the descent angle from the MDA of 560 feet, is 4.7 degrees.Footnote 113 If flight crews choose to land when they reach the MAP, at MDA, the resulting descent path would be steep and lead to a rate of descent of approximately 1240 fpm. Under industry accepted stable approach criteria, this would be considered unstable, as it is greater than 1000 fpm. Therefore, any decision to land should be made prior to the MAP in order to maintain an approximate 3-degree approach path and remain on a stable approach.
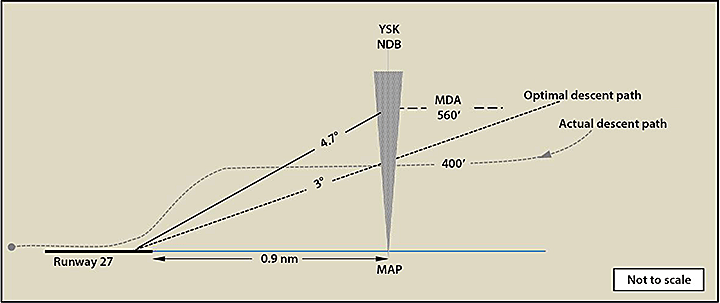
1.18.3.2 Instrument approaches for CYSK
As with many small airports, CYSK had only 1 non-precision NDB approach (Runway 27) with the option of circling to the opposite runway (Runway 09).In February 2014, NAV CANADA issued 2 new RNAV (area navigation) GNSS approaches for CYSK, 1 for Runway 09 and 1 for Runway 27. ICAO defines area navigation as a method of navigation that permits aircraft operation on any desired flight path within the coverage of ground or space-based navigation aids or within the limits of the capability of self-contained aids, or a combination of these.Footnote 114 With RNAV approaches, pilots have the option of straight-in approaches and localizer performance with vertical guidance (LPV) capability. This offers better situational awareness than conventional NPAs thereby reducing the risk of an ALA. The 2 new CYSK approaches include LPV minima that provide both lateral and vertical guidance to 250 feel agl. The NDB Runway 27 approach is still available.
Changes to the approach chart depiction were put into effect for various reasons, one of which was the need to be in line with Flight Safety Foundation (FSF) principles and ICAO guidance material. Changes to the approach charts were not in response to this accident.
Since 2010, Perimeter worked with the Manitoba Aviation Council (MAC), Northern Air Transport Association (NATA), and sat as a member on the NAV CANADA Advisory Committeewith the sole purpose of requesting that NAV CANADA design GNSS approaches at busy northern airports. The design of GNSS approaches is ongoing.
1.18.4 Approach and landing accidents
In 1996, the FSF formed it's Approach-and-Landing Accident Reduction (ALAR) Task Force. By focusing on approach and landing, the task force was able to work outside the strict definition of CFIT accidents, which does not include landing short or long, runway overruns, or loss of control following an unstable approach. In 1998, the FSF task force issued recommendations targeting the reduction and prevention of ALAs.The statistical data collected by the FSF ALAR Task Force at that time revealed that ALAs represented approximately 55% of total hull losses and 50% of fatalities. The flight segment from the initiation of the approach to the completion of the landing roll represented only 4% of the flight time but 45% of hull losses. CFIT (including landing short of the runway), loss of control, runway overrun, runway excursion, and unstable approaches are the 5 types of events that account for 75% of approach-and-landing incidents and accidents.
Although the majority of the statistics cited by the task force are pertinent to this occurrence and operation, several statistics cited in the study stand out as being particularly applicable to this event:
- CRM issues, including decision making under stress, are observed as circumstantial factors in more than 70% of ALAs.
- More than 70% of ALAs contained elements that should have been recognized by the crew as improper and should have prompted a go-around.
- When an unstable approach warrants a go-around decision, less than 20% of flight crews actually initiate a go-around.
- Continuing an unstable approach is a causal factor in 40% of all ALAs.
- Approximately 70% of rushed and unstable approaches involve an incorrect management of the descent-and-approach profile and/or energy level (i.e., being slow and/or low, being fast and/or high).
- The risk of an ALA is higher in operations conducted in low light and/or visibility, on wet or otherwise contaminated runways, and with the presence of optical or physiological illusions.
- The lack of acquisition or the loss of visual references is the most common primary causal factor in ALAs.
Results of this study and analysis presented at the FSF Forum in Belgium indicated that
- between 3 and 4% of all approaches are reported/recorded as unstabilized;
- only 3% of these results in a go-around being flown; and
- 97% of unstabilized approaches continue to be flown to a landing contrary to SOPs.
- had degraded representations and awareness of the situation;
- were more tolerant of deviations from operational limits and procedures;
- were less likely to perform required checklists and calls; and
- were less likely to take advantage of other crew members or seek their advice about the best course of action.
Because their situational awareness was dimmed, the pilots (in the study) who chose to continue on an unstable approach, experienced not seeing certain threats (anticipatory awareness) such as aircraft instabilities; weather and aircraft configuration; selectively leveraging their ‘stick and rudder' experiences (critical awareness) as permission to continue; and finally, perceiving or assuming crew dynamics (relational awareness) to support non-compliant behavior.The TSB report on its investigation into a CFIT occurrence in Quebec in December 2009 (A09Q0203) cited information relevant to the FSF's ALAR task force findings and recommendations. The recommendations are reiterated in this report as they remain applicable to the circumstances surrounding this occurrence (Appendix H).
The TSB database shows that in 2012 in Canada, there were 34 ALAs; 3 of these were operating under Subpart 705; 4 were operating under Subpart 704; and 16 were operating under Subpart 703. The other 11 occurrences were in the ‘other commercial operations ALAs' category.
The FSF ALAR task force determined that the risk of ALAs was 5 times higher for non-precision approaches than for precision approaches.
1.18.5 TSB Watchlist
Approach-and-landing accidents are a 2014 TSB Watchlist issue. The Watchlist is a list of issues posing the greatest risk to Canada's transportation system; the TSB publishes this list to focus the attention of industry and regulators on the problems that need addressing today. As this occurrence demonstrates, landing accidents continue to occur at Canadian airports.1.18.6 Flight Safety Foundation Approach and Landing Accident Reduction Tool Kit
In addition to the recommendations put forth by the FSF ALAR Task Force in 1998, the FSF developed and distributed an ALAR Tool Kit. It is a resource that can be modified as required to fit the particulars of an operation, and it can also be used for training in the various positions within a company. The objective of the tool kit is to help highlight, evaluate, and mitigate the associated risks of a flight before departure. If the risk level is deemed too high after using the tool kit checklist, then the flight could be turned down or delayed until risks are mitigated to maintain an acceptable level of safety. Although promoted, and its use encouraged by TC,Footnote 117 many Canadian operators are not aware of the existence of the FSF ALAR Tool Kit, or if aware of it, are not using it. Perimeter, although aware of the tool kit, had not used it, nor was it mandatory to do so.1.18.7 Go-around – Flight Safety Foundation European Advisory Committee
1.18.7.1 General
An article in Aviation International NewsFootnote 118 stated that the FSF European Advisory Committee's results, after analysing 66 go-around related accidents that occurred between 2002 and 2013, showed that the go-around itself was usually the consequence of something that went wrong on the approach. Several trends were noted:- Significant procedure non-compliance was likely to precede the go-around attempt;
- In half of the fatal accidents, there was significant violation of approach minima;
- Nearly three quarters of all go-around decisions were made when the aircraft was below 500 feet agl;
- In 5 out of 10 fatal accidents, the PF flew below minimums with little negative input from the PNF;
- Most of the go-arounds were flown manually by the PF.
Most missed approaches are executed due to bad weather conditions and require particular attention in order to immediately transition back to flying with reference to the instruments. The procedure may be further complicated if airspeed and/or thrust settings are low.Footnote 119
1.18.7.2 Go-around training
Go-arounds are not common and, therefore, can entail some risk. One in 10 go-around attempts has a potentially hazardous outcome, including exceeding aircraft performance limits. Go-around manoeuvres are often flown poorly and are more likely to be fatal than common runway excursion accidents.Footnote 120Perimeter flight crews practice go-around procedures in a static flight training device prior to initial training on the aircraft. These procedures are also trained during every initial and recurrent aircraft training session. A minimum of 2 missed approaches in the recurrent training and an average of 5 to 6 missed approaches in an initial training program are conducted. At least 1 missed approach is conducted at altitude, simulating an engine failure at the point of go-around. A 2-engine go-around at a very low altitude (balked landing) following a circling manoeuvre may also be conducted during training.
1.18.7.3 Low-energy training
Following the TSB investigation of a Canadair CL-600-2B19 loss of control on go-around (rejected landing) occurrence in New Brunswick in December 1997 (TSB Aviation Investigation Report A97H0011), the Board recommended that:The Department of Transport ensure that pilots operating turbo-jet aircraft receive training in, and maintain their awareness of, the risks of low-energy conditions, particularly low-energy go-arounds.Under existing regulations (CAR 704.115), air carriers operating under Subpart 704 shall establish and maintain a ground and flight training program which includes low-energy awareness training (CASS 724.115 (34)). This training requirement, however, applies to turbojet aircraft operations only, and does not include turboprop aircraft such as the Metro III.TSB Recommendation A99-06
On 13 May 1998, TC issued Commercial and Business Aviation Advisory Circular (AC) No. 141 to notify pilots and air operators of the potential hazards associated with a balked landing or go-around. The circular states that, “an aircraft is not certified to successfully complete a go-around without ground contact once it has entered the low-energy landing regime.”
The AC also advises that air operators should immediately ensure that their pilots and training personnel are aware of the hazards associated with low-energy go-arounds, and verify that their training programs address these hazards and provide procedures for dealing with them. The AC does not distinguish between training aimed at operators of turbojet aircraft and turboprop aircraft.
Executing a low-energy go-around is a demanding manoeuvre and is often accompanied by additional stress. Although periodically practised in simulator training, executing a low-energy go-around in real life situations is a rare event.
Perimeter does not address low-energy rejected landings for the Metro II or III in flight training or in simulator training. However, a simulated visual missed approach at altitude is practised . The aircraft is allowed to slow for landing, then a go-around is conducted using the go-around procedure; a full-flap, gear-down configuration is used, in a slow airspeed situation, with an engine failure. This exercise allows the candidate to execute the procedure and it demonstrates degraded aircraft performance.
1.18.7.4 Putting go-around information to good use
The FSF Go-Around Forum found that for better go-around decision making to happen, pilots need to- enhance crew dynamic situational awareness;
- have better refined and defined go-around policy (stable approach parameters and stable approach height);
- be better guided by SOPs, which helps minimize the subjectivity of the go-around decision;
- obtain improved go-around training, including the recognition of threat factors and difficulties associated with the go-around decision. Go-around training should include execution from other-than-decision height, MDA or designated stabilized approach gate.Footnote 121 Also, training must keep in mind that the majority of go-arounds are made because of weather (forward visibility, ceiling, wind velocity, and turbulence).
1.18.8 Aircraft performance
The TSB laboratory looked at the aircraft performance effects of raising the landing gear during the go-around. The landing gear was selected UP immediately upon the go-around call, which is earlier than specified in the AFM balked landing procedure. The wreckage indicates that the gear was in the process of retracting when the aircraft collided with terrain.Given the available data, it was not possible to quantify the effects upon performance and trim/control throughout the full retraction cycle, but the effects can be discussed in general.
When the landing gear is retracted, the total aerodynamic drag of the aircraft is reduced, allowing greater acceleration and rate of climb. The published performance data for balked landing conservatively assumes that the landing gear remains extended. Retracting the landing gear should further increase the aircraft's climb and acceleration capability compared with the published performance.
Airworthiness certification requires that raising of landing gear be a smooth transition that does not have an unacceptable effect on aircraft control and trim in normal and emergency situations. It is therefore expected that the action of raising the landing gear would not diminish the ability to execute the published balked landing procedure. The manufacturer confirms that there is a negligible change in aircraft pitch when retracting the landing gear.
Therefore, raising the landing gear earlier than specified in the published procedure is expected to have had no detrimental effects upon controlling the aircraft or achieving the published balked landing performance.
1.19 Useful or effective investigation techniques
Not applicable.2.0 Analysis
2.1 General
The analysis will focus on the circumstances affecting the flight and the factors that could have led the crew to deviate from learned procedures and regulations, to descend below minimum descent altitude (MDA) before acquiring the required visual references, and to miss critical cues warranting the initiation of a missed approach.Additionally, the analysis will address the lack of readily available data on the number of infant and child passengers travelling by air, and the lack of regulations for the mandatory use of suitable restraint devices that would provide an equivalent level of safety for infants and children compared to adult passengers.
2.2 Weather
Weather obtained for flight planning, although marginal, was forecast to be above minima for the approach at Sanikiluaq (CYSK), and the weather forecast for Kuujjuarapik (CYGW) was appropriate for its use as an alternate airport. The captain had verified weather prior to departure and knew of the low pressure system expected to pass through the area of CYSK that afternoon, and that the same weather system would affect the airports located to the east of Hudson Bay. Weather, at the time of planning, was not seen as a threat; ceilings and visibility were above the published minima.While the aircraft was preparing for takeoff, the aviation routine weather reports (METAR) for CYGW deteriorated, and the aerodrome forecast (TAF) was amended at 1936 UTC. The amended TAF forecasted weather below approach minima during the initial period, but improving to 2 statute miles (sm) visibility and overcast cloud at 1500 feet above ground level (agl) prior to the estimated time of arrival at the alternate. The crew did not obtain this updated weather forecast.
During the flight, the METARs showed poor weather consistent with the initial forecast period. The TAF for CYGW was amended again at 2211 UTC, and this time the forecast improvement of 2 sm visibility and overcast cloud at 1500 feet agl was delayed until 2400 UTC, making CYGW unsuitable as an alternate.
As forecast weather was initially not deemed a threat, the crew did not obtain updated weather for destination and alternate airports while en route, and were surprised, upon obtaining an update prior to descent at CYSK, that weather at CYGW was below minima for the approach. The 2200 UTC METAR for CYGW had dropped to ½ sm in snow with a vertical ceiling of 400 feet. This weather activity was occurring during the en-route portion of the flight. The crew received the 2200 UTC METAR at 2228 UTC. This was the first time the crew realized the weather at the alternate was below approach minima. The crew was surprised by the low weather conditions in CYGW, and also realized that a forecast improvement in the weather would only occur shortly after the estimated time of arrival at the alternate airport. Upon realizing the weather at the alternate was no longer favourable for landing, the crew discussed using La Grande Rivière (CYGL) as an alternate if a landing at CYSK was not possible. However, total fuel on board at that time did not accommodate this option. This likely increased the pressure to land at CYSK.
The winds were favouring an approach to Runway 09; however, CYSK did not have a published instrument approach procedure for this runway. The weather did not allow for visual manoeuvring to Runway 09, and the crew decided to land on Runway 27 with the associated risks of landing with a 14-knot tailwind on a 3807-foot runway. Lack of a published instrument approach for Runway 09 led to the crew's decision to attempt a downwind landing.
2.3 Human performance issues
2.3.1 Cumulative effects of frustration, fatigue and stress
The number of MEDEVAC and charter flights to areas in Nunavut on 22 December was greater than the number of Canada Air Pilot instrument approach charts available to Perimeter flight crews. The chosen solution to this problem was to pick up the necessary documents at the Keewatin Air hangar where the passengers were to embark. This meant, however, that the approach chart information was not available for pre-flight preparation.Under Type B operational control, dispatch would have a responsibility to find a way to provide the necessary charts, chart information (copy), or to cancel the flight. Under Type C, the captain has that responsibility. The lack of charts was an operational shortfall and an irritant for the captain. This placed pressure on the captain to develop a work-around solution in a short period of time; a solution that would entail cancelling the flight, delaying the flight, or proceeding without the necessary publications until just prior to departure. The captain chose the third option as it had the least impact on operations.
Shortly after takeoff, the captain realized the instrument approach charts had been forgotten and chose not to return to Winnipeg (CYWG), as this would have resulted in further delay and necessitated addressing dispatch and management about extending the duty day or finding a replacement crew. This also would have had a negative impact on operations.
The crew had received some of the approach chart information via radio from another pilot. However, without reference to the actual chart, the crew did not have a visual reminder of altitude limits or approach diagrams to assist with orientation of the aircraft in time and space. This made the crew more susceptible to error and loss of situational awareness, such as the incorrect direction of the procedure turn and incorrect turn on the missed approach.
The lack of required flight documents, such as instrument approach charts, placed pressure on the captain to find a work-around solution during flight planning, and negatively affected the crew's situational awareness during the approaches at CYSK.
If instrument approaches are conducted without reference to an approach chart, there is a risk of weakened situational awareness and of error in following required procedures, possibly resulting in the loss of obstacle clearance and an accident.
Several unforeseen issues arose during the flight preparation, which likely had a negative effect on the crew's mental readiness for the flight. The aircraft did not have the required survival kit and this had to be obtained at the Keewatin Air hangar and properly stowed. The single redline limit minimum equipment list (SRL MEL) deferred maintenance issue was due to expire at midnight local time that night (0600 UTC on 23 December 2012). There was also the delay caused by the replacement of the cargo door handle position switch, which necessitated a re-filing of the flight plan. The change to the cargo load resulted in a change of fuel quantity and subsequent choice of alternate airport. All of these created additional work for the crew in this Type C dispatch environment. As the delay for departure was extended, the flight crew duty day was being stretched. Any additional extension to the duty day would have had to be addressed with management.
Although delays and changes in scheduling and logistics are not uncommon in airline operations, frustrations can arise if crews do not feel they have control over operational matters, and if they feel that the company is not providing support. Increased levels of frustration can decrease performance and increase risk-taking behaviour; behaviours that would not normally be present under other circumstances.
As described in the company operations manual (COM), dispatch does not provide the same assistance to Subpart 703 or 704 flight crews. The type of services offered by dispatch to Subpart 705 flight crews would reduce the workload of Subpart 703 and 704 crews during pre-departure planning. These services likely would have reduced the occurrence crew's workload and stressors related to scheduling changes.
The captain felt frustrated as a result of the pre-flight preparation issues, and it is evident from analysis of his speech that signs of frustration persisted after takeoff. The captain's use of 43 expletives in conversation with the first officer (FO) during the non emergency, non stressful, 2-hour period preceding the occurrence, showed a rate of approximately 21.5 swear words per hour. This type of behaviour was seen as being out of character for the captain.Footnote 122
The long day and circadian rhythm timing at the time of the occurrence may have had a compound effect, adding to the level of fatigue resulting from acute sleep disruption. Based on the captain's 1.5-hour wake period and resultant shortened sleep duration the night before the occurrence, acute sleep disruption may have played a role in the captain's behaviour during the flight by increasing the risk for fatigue and its associated performance decrements. The FO did not experience the same sleep disruption; therefore, fatigue was not considered as high a risk factor.
The weather was worse than anticipated and created difficulties in visually acquiring the runway environment and aligning the aircraft to land. The excursions in controlling altitude and airspeed were likely due to an increased stress level, and added to the sense that the situation was deteriorating. Additionally, the weather at the alternate airport was reported to be worse than at CYSK. All these factors would have increased the level of stress and workload as the crew attempted to solve their predicament.
Increased stress levels can adversely impact a pilot's ability to perceive and evaluate cues from the environment, and may result in attentional narrowing. This may result in pilots paying attention only to certain cues while excluding others, which in turn leads to a loss of situational awareness. Under extremely stressful conditions, this can lead to an unintentional shift away from well-learned, highly practised, essentially automatic actions. The crew was very focused on landing the aircraft at CYSK, and an increase in workload and stress during the instrument approaches resulted in attentional narrowing and a shift away from well-learned, highly practised procedures.
2.4 Crew resource management
2.4.1 Crew resource management training standards
Transport Canada (TC) standards for crew resource management (CRM) training are based on outdated concepts. This has been discussed in previous TSB investigation reports, most recently the Boeing 737-210C controlled flight into terrain (CFIT) occurrence in Resolute Bay, Nunavut (TSB Aviation Investigation Report A11H0002). Although TC is in the process of developing a new training standard, one that will apply to Subpart 702, 703, 704, and 705 operations, the changes have yet to be promulgated.As stated in the Safety Concern highlighted in TSB report A11H0002, until such time as the new regulatory framework for CRM training is in place and its effectiveness is validated, there remains a risk that flight crews may not routinely practice effective CRM.
If TC CRM training requirements do not reflect advances in CRM training, such as threat and error management (TEM) and assertiveness training, there is an increased risk that crews will not effectively employ CRM to assess conditions and make appropriate decisions in critical situations.
2.4.2 Training received by the crew
The flight was operated under Subpart 704 of the Canadian Aviation Regulations (CARs); as such, CRM training was not required. The company was required to provide CRM training to its crews that operate aircraft under Subpart 705, and had elected to extend this training to its Subpart 703 and Subpart 704 crews as well. The FO had received this training. The captain had received CRM training while working for a different operator. Training provided by Perimeter is in line with TC CRM training requirements for Subpart 705 operations.2.4.3 Crew resource management during the approaches
2.4.3.1 Initial approach plan
As the crew discussed the fuel remaining and weather at the possible alternates, they realized that they had enough fuel only for the flight-planned alternate, which was below approach minima at the time they were descending to commence the initial approach at CYSK. Multiple approaches at CYSK was considered as a plan of action rather than diverting to the alternate airport; however, the crew did not commit to a particular plan as they likely expected to land at CYSK given that weather was above approach minima.The captain briefed that the initial plan would be a straight-in visual approach to Runway 09 and, if the runway was not visible, that they would continue direct to the YSK non-directional beacon (NDB) for an NDB approach to Runway 27.
The lack of an instrument approach to one of the two runways resulted in the crew not having the option of landing into wind without conducting a circling manoeuvre. This, combined with the unsuccessful attempt at circling, led the crew to accept a strong tailwind approach and landing on Runway 27.
The approach briefing included the procedure turn altitude and distance, but did not include whether the procedure turn would be executed north or south of the inbound track. The FO queried the direction for the procedure turn; however, the discussion went on to the targeted altitude, and no response was given. The global positioning system (GPS) was used to determine distance from the NDB.
The missed approach was briefed as runway heading to minimum safe altitude (MSA). A decision on what course of action to take afterwards was deferred. Missing from this briefing was the final part of the published missed approach instruction, a right turn back to the YSK NDB. Some of these errors were likely due to the lack of an instrument approach chart.
Furthermore, no decision had been reached regarding what the crew would do at the missed approach point (MAP) for Runway 27, i.e., land or circle for Runway 09. The crew had discussed the possible effects of landing on Runway 27 with a tailwind, but there was no confirmation of any of the circling considerations. Circling was confirmed only once the runway was visible.
The crew were expecting to acquire visual reference with the ground during the approach to Runway 27 as the cloud ceiling and visibility were reported to be above minima for the approach. This may also explain why the aforementioned items remained unresolved.
The cold temperature correction was considered and applied to the minimum descent altitude (MDA) for NDB Runway 27 and the other procedure altitudes. Corrections were not made to the circling MDA since it had not been obtained. Although not required by regulations, if temperature corrections are not applied to all altitudes on the approach chart, there is an increased risk of CFIT due to a reduction of obstacle clearance.
2.4.3.2 First approach to Runway 27
On arrival in the vicinity of the CYSK airport, the runway was not visible and the crew commenced the NDB Runway 27 approach. The captain executed a teardrop turn to the right, opposite to the published direction. However, since the crew used the 25 nautical miles (nm) altitude, obstacle clearance was provided.As the aircraft approached the MDA on the inbound track, the crew saw the lights from the town and, shortly after, the runway. The aircraft was not in a position to land on Runway 27, so the captain initiated a circling procedure for Runway 09, and the FO concurred.
2.4.3.3 Circling procedure following first approach to Runway 27
The captain was the pilot flying (PF) and the FO was the pilot not flying (PNF). In a circling procedure, the PF must maintain visual reference with the runway as well as the published circling altitude to ensure obstacle clearance. The PNF monitors the instruments and advises of any airspeed and altitude deviations. The crew did not have the approach chart and had not received the circling minimum altitude of 620 feet; the captain chose to maintain 500 feet above sea level (asl) while circling, although 600 feet asl had been briefed and set on the altimeter.Shortly after initiating the circling procedure, the captain lost visual reference with the runway. A missed approach must be initiated when visual reference is lost; however, the crew continued to circle in instrument meteorological conditions (IMC). At this point, it was no longer a circling procedure, but rather a manoeuvre to position the aircraft to regain visual contact with the runway. At one point during this manoeuvre, the aircraft was as low as 155 feet agl. As the aircraft was returning towards the airport at an altitude of approximately 400 feet asl, the captain saw the runway, but again the aircraft was not in a position to land.
During the circling for Runway 09, signs of stress interfering with crew performance and CRM were displayed. Communication calls were omitted or not responded to, flight parameter corrections were not initiated or made at all, decision making was altered, and deviations from regulations and procedures occurred. Missed opportunities to manage threats and errors are a known reaction to stress. The accumulation of mismanaged threats and errors affected the level of stress experienced by the crew, and likely resulted in the required missed approach procedure not being executed when visual contact with the runway was lost during the circling procedure to Runway 09. Not initiating a missed approach at the point where visual reference to the runway was lost during the circling increased the risk of CFIT.
2.4.3.4 Second circling procedure
The crew decided to initiate a circling procedure for Runway 27. During the initial stage of this manoeuvre, there were excursions in altitude and airspeed:- Climb from 400 feet asl to 900 feet asl;
- Descent from 900 feet asl to 560 feet asl;
- Airspeed 140 knots indicated airspeed (KIAS) to 160 KIAS.
The captain lost sight of the runway again and initiated a missed approach in the vicinity of the YSK NDB. If it becomes necessary to conduct a missed approach after starting visual manoeuvres, the Instrument Procedures ManualFootnote 123 recommends a climb be initiated followed by a turn back to the centre of the airport. The aircraft should then be established as closely as possible on the missed approach procedure track for the approach flown (NDB Runway 27). Although the published missed approach procedure for Runway 27 was not followed, the crew flew a wide arcing left turn to the YSK NDB, climbing to the minimum 25 nm safe altitude. This was not fully in accordance with the recommended procedure; however, obstacle clearance was assured.
Twice in quick succession the FO reminded the captain that the altitude was 1600 feet, but the captain responded 1500 feet. The FO did not correct the error. This is another indication of unresolved communications.
2.4.3.5 Second NDB Runway 27 approach
During the second approach, there were indications of the crew deviating even further from learned procedural norms and regulations:- The procedure turn was flown at 1500 feet asl versus the briefed 1600 feet asl.
- The descent was 197 feet below published MDA without the required visual reference.
- Despite being high in relation to the runway threshold when visual references were established, the final descent was delayed.
- Excessive airspeed (VREF + 30) and rate of descent (>1800 feet per minute) were used once the decision to land was made.
- The threshold crossing height was high (approximately 180 feet agl).
The runway was sighted when the aircraft was approximately 0.7 nm from the threshold at a height of 253 feet agl (400 feet indicated). The captain called for full flaps 1 second after sighting the runway. The FO performed the remaining landing checklist items with no call or response from the captain. This omission of the required responses is evidence of task saturation and stress.
The captain flew beyond the MAP without visual reference to the runway although, procedurally, a missed approach was warranted. This was likely a conscious decision based on late sighting of the runway on the previous approach and lack of an alternate option. The crew felt pressured to land on this approach.
The descent for landing was initiated late. Engine power was decreased to idle 10 seconds after visual reference was acquired. It is not known why there was a delay between sighting the runway and initiating the descent. It is possible that the captain was starting to see some of the runway environment, but was not yet comfortable that there was sufficient visual reference to initiate the descent.
As a consequence, the aircraft had less distance in which to descend and a steeper approach angle was required to execute the landing within the confines of the runway. This resulted in a high rate of descent (>1800 ft/min) and high airspeed (150 knots) as the captain tried to reach the threshold of the runway. This attempt was exacerbated by the high ground speed due to the high airspeed and the strong tailwind. The final descent was initiated beyond the MAP and, combined with the 14-knot tailwind, resulted in the aircraft remaining above the desired 3-degree descent path.
During this landing attempt, the first ground proximity warning system (GPWS) PULL UP warning was generated as the rate of descent exceeded 1800 ft/min. The aircraft approached the threshold of the runway at a height of approximately 180 feet agl and an estimated ground speed of 159 knots. The GPWS warning continued until the aircraft was approximately 900 feet past the threshold at a height of approximately 60 feet agl. The captain was focused on the landing despite the growing instability of the approach. The captain no longer had the overall perspective of the extent to which the approach and chance of landing safely had deteriorated.
The FO was monitoring airspeed and calling deviations, but did not express concern regarding aircraft speed and height at the threshold. The FO had also lost perspective regarding the aircraft's state and the developing risks associated with the approach.
Both the captain and FO were concentrated on a very specific aspect of the approach, and lost sight of the threat associated with the high sink rate and airspeed as the aircraft crossed the threshold. This, and the lack of response to the GPWS warnings, are indications of attentional narrowing.
Both pilots were focused on landing the aircraft to the exclusion of other indicators that warranted alternative action.
2.5 Stable approach criteria
Company standard operating procedures (SOP) did not provide detailed criteria for stabilized approaches or guidance for action to take in the event of an unstable approach. The SOPs mention that the rate of descent should not be greater than 800 ft/min below 1000 feet agl.Section 1.17.8 of the SOPs describes criteria that characterize a stable approach. Approaching the threshold of Runway 27 at approximately 180 feet agl, the aircraft was unstable in several of these parameters:
- Rate of descent: above 1800 ft/min
- Speed: VREF + 25
- Throttles: idle.
This instability on final approach contributed to the aircraft being half-way down the runway with excessive speed and altitude.
The aircraft was not in a position to land and stop within the confines of the runway, and a go-around was initiated.
2.6 Descent technique for non-precision approaches
The CYSK non-precision approach is designed such that a descent from the MAP at MDA results in a steeper-than-optimum descent path. If visual references are not acquired until close to the MAP, at MDA, crews may be tempted to intiate a steep, unstable descent to the threshold in order to land. If the MAP on non-precision instrument approaches is located beyond the 3-degree descent path, there is an increased risk that a landing attempt will result in a steep, unstable descent, and possible approach-and-landing accident.2.7 Rejected landing
2.7.1 General
At the time of the captain's go-around call, the aircraft was considered to be in a low-energy landing regime because of the following parameters:- The aircraft was below 50 feet over the runway;.
- Gear and flaps were in landing configuration.
- Thrust was at idle and airspeed was decreasing.
At the time of the go-around call (10 seconds prior to impact), the FO was busy setting power and reconfiguring the aircraft as per procedure. These actions could preclude the monitoring of airspeed and vertical speed at a critical phase of flight. Any reduction of pitch during this transition period reduces the ability of the aircraft to establish a positive rate of climb.
The manufacturer's balked landing procedure requires confirmation of a positive rate of climb prior to retracting the gear and setting the flaps. This ensures the aircraft is safely climbing away from the ground before initiating any other actions.
After re-configuring the aircraft, the FO made a speed call (105 knots). The airspeed was therefore below the target climb speed of 110 knots. The low speed call may have prompted the captain to unintentionally release back pressure on the control column to accelerate to the desired average target climb speed. This would be a normal reaction to a low speed call in a climb attitude; however, it may not be appropriate given that the aircraft was attempting to clear terrain. It is also possible that the captain's visual scan was momentarily diverted from the attitude indicator to the airspeed indicator at a time when pitch attitude was critical. A slight release of the control column would likely have been sufficient to stop a positive rate of climb. The aircraft struck terrain 4 seconds after the speed call.
The configuration change at a critical phase of flight, possibly combined with a slight pitch reduction, may have contributed to the aircraft's poor climb performance. A rate of climb sufficient to ensure clearance from obstacles was not established, and the aircraft collided with terrain.
2.8 Cabin safety
2.8.1 In-cabin seating
2.8.1.1 Passenger seating location
As with all Perimeter flights in the Metro III, there was no pre-arranged seating for this flight, and passengers were free to choose their own seat. The Metro III affords little leg room between seats, the aisle is narrow, and there are no overhead bins to store carry-on baggage. Seat 1L is the seat that has the most leg room, and the main doorstair which folds into the cabin is situated immediately in front of it. The mother holding the infant chose to sit in seat 1L and had not been directed to sit elsewhere, although she was responsible for another. Without a seat back in front of seat 1L, the mother would not have been able to adopt the recommended bracing position had it been commanded. Additionally, the lack of a seat in front of the mother meant there was limited energy-absorbing material in front of her and her infant. Furthermore, the aircraft main doorstair was positioned directly in front of her seat, creating a hazard for the infant.The absence of an energy-absorbent seat back in front, combined with the presence of the hard, sharp, metal stairs, ceiling and cockpit partitions, likely resulted in the lap-held infant coming into contact with hard, non-deformable interior surfaces during the dynamics of the impact sequence.
If a person holding an infant is seated in a row with no seat back in front of them, there is an increased risk of injury to the infant as no recommended brace position is available.
2.8.1.2 Emergency exit seating
Both Perimeter's safety features card and TC define the main door of the aircraft as an emergency exit. Company practice in regards to the seating of passengers assisting others next to the main exit was inconsistent with this definition. Perimeter's interpretation of the definition of an emergency exit meant that, on occasion, occupants assisting another person might have been sitting in seat 1L. Seating a passenger who is responsible for another in a seat adjacent to an emergency exit could adversely affect the safety of passengers or crew members during an emergency evacuation.In this occurrence, egress took place via the forward right overwing exit. The main door could not be opened due to damage incurred during the impact with the ground. The presence of the infant's mother next to the main door exit did not hinder the evacuation of the other occupants.
If a person assisting another is seated next to an emergency exit, there is an increased risk that the use of the exit will be hindered during an evacuation.
2.8.2 Passenger briefings
No individual passenger briefing was given to the mother of the infant before takeoff. Company procedures and training regarding individual briefings and briefing content were lacking. Amongst other items, the briefing should include how to hold the infant for takeoff and landing. Although the mother of the infant had not been given an individual safety briefing prior to this flight, she had travelled often with her other children, and held her infant as described by the safety features card and as instructed in previously provided briefings. The lack of an individual briefing for the occurrence flight did not directly affect the safety of the infant.2.8.3 Restraint systems
2.8.3.1 Carry-on baggage control programs
Much effort, time and money is put into air carrier carry-on baggage control programs, which are required by TC. Carry-on baggage programs applicable to Subpart 705 operations include ensuring that baggage remains under a certain weight and size, and that it is safely stowed during all phases of flight. Similar requirements for restraining carry-on baggage apply to Subpart 703 and 704 operations under CAR 602.86. Additionally, TC has emphasized the importance of ensuring that passengers wear seatbelts at all times, and cabin crew are directed to restrain all cabin equipment in case of sudden, unexpected in-flight turbulence.2.8.3.2 Restraint of young children
Research has shown that, due to anthropomorphic differences (i.e., body proportions including height, weight, head size, and pelvic development) between adults and children, the standard lap belt is not suited for the safe restraint of small children. A child may either slip under the seatbelt to the floor, or sustain severe abdominal injuries in the event of in-flight turbulence or an emergency landing. Furthermore, given their smaller size, a young child may be unable to assume the recommended brace position for adults. If young children are not adequately restrained, there is a risk that injuries sustained will be more severe.2.8.3.3 Infant restraint
Biomechanical research has found that, due to limitations in human clasping strength, it is not always possible for adults to restrain children adequately in their laps by holding onto them. Infants are therefore exposed to undue risks of injury when seated on an adult's lap. Much effort and many recommendations have been made, particularly by the National Transportation Safety Board (NTSB), to mandate the use of age- and size-appropriate child restraint systems (CRS) for children and infants. However, in most countries around the world, including Canada, infants are not required to be restrained in an age- and size-appropriate CRS at any time during a flight. Despite publishing safety information on in-flight turbulence events and the risk of death or injury to passengers if objects are not restrained, TC has not changed the regulations concerning the requirements for CRS for infants.In this occurrence, the infant passenger was not restrained in a CRS, nor was one required by regulations. The infant was ejected from the mother's arms during the impact sequence, and contact with the interior surfaces of the aircraft contributed to the fatal injuries.
Infants are not required to be restrained at any time during a flight. If a lap-held infant is ejected from its guardian's arms, there is an increased risk the infant may be injured, or cause injury or death to other occupants.
At present, TC does not anticipate making any changes to the regulations for the use of CRS for infants or young children. For now, TC recommends the use of CRS on board aircraft, but defers to the air carriers to educate the travelling public and promote their use. Therefore, infants and young children do not benefit from an equivalent level of safety compared to adult passengers.
2.8.4 Lack of data regarding infant and child passengers
The Transportation Information Regulations do not currently require operators to gather or provide to the Minister of Transport information on the number or ages of children and infants travelling by air. Infants are not included in the total passenger count when secured in a lap-held position by a parent or guardian passenger. Data collected on the number of passengers do not separately identify children under 12 years old and, therefore, this information is not easy to extract from the total passenger count. As a result, it is difficult to properly assess infant and child passenger exposure to air travel.International Civil Aviation Organization (ICAO) and TC statistics show that passenger travel is on the rise; however, the proportion of child or infant passengers is not available. Information supplied by Perimeter and 3 other air carriers indicated that infants and children make up nearly 14% of their total passenger loads.
Risk assessment exercises and safety initiatives are data-driven. Without adequate data collection, the exposure to risk for this population of individuals cannot be adequately assessed. The number of children and infants travelling with these carriers could be higher than for carriers servicing destinations in the southern part of the country, as air travel for residents of northern communities is often the only means of travel. Nonetheless, an equivalent level of safety should be provided for any traveller regardless of age.
Additionally, better data collection is needed on the age, size, use of restraints, and injury patterns for infants and children, to better assess their risk exposure and to assist in the development of effective restraint systems for these travellers. The TSB cannot analyse trends without data.
If more complete data on the number of infants and children travelling by air are not available, there is a risk that their exposure to injury or death in the event of turbulence or a survivable accident will not be adequately assessed and mitigated.
2.9 Organizational issues
2.9.1 Company ground proximity warning system training
In the company operations manual (COM) and the airplane flight manual (AFM), sounding of the GPWS warning requires immediate pull-up action. However, the SOPs do not provide standard calls and responses or necessary actions to take in the event of a warning. If there is not sufficient guidance in the SOPs, there is a risk that crews will not react and perform the required actions in the event that GPWS warnings are generated.2.9.2 Airplane flight manual procedure for blaked landing versus standard operating procedures for go-around
The company SOPs contain a single procedure for a 2-engine go-around, regardless of energy state or stage of approach and landing. Although the SOP does not include consideration for a balked landing from a low-energy landing regime, training with this SOP was conducted during go-arounds from a low-energy state.The procedure calls for raising the flaps at a critical transition from a landing attempt (close to the ground) to a stabilized climb, and contributed to an insufficient climb gradient to ensure obstacle clearance.
The AFM has a separate procedure for a balked landing to address this critical phase of flight.
If SOPs, the AFM and training are not aligned with respect to low-energy go-arounds, there is a risk that crews may perform inappropriate actions at a critical phase of flight.
2.9.3 Safety case
The company's safety case process was developed as a proactive tool to identify and mitigate risks. Identification of risk factors allows for better situational awareness and better planning prior to departure, and assists in the effective management of such risks. However, as constructed, the process is an arduous one involving several company representatives, which does not accommodate impromptu requests for charter flights. Operations to CYSK were frequent enough that the company did not regard the request for the charter as a new destination; therefore, a safety case was not conducted.2.9.4 Extra fuel
The investigation determined that an additional 200 pounds of fuel had been loaded on the aircraft as a safety buffer in case of unexpected delays. The practice of loading extra fuel was known within the company. As was the case in the occurrence flight, this may mean that the manufacturer's approved maximum take-off weight for the aircraft is exceeded by this 200-pound additional fuel load. The additional weight did not play a role on aircraft performance during the approach, landing or go-around at CYSK. The fuel consumed during the 3-hour flight resulted in the total weight being well below maximum gross weight. If additional contingency fuel is not accounted for in the aircraft weight, there is a risk that the aircraft may not be operated in accordance with its certificate of airworthiness or may not meet the certified performance criteria.2.10 Transport Canada oversight
Perimeter had not found it necessary to complete a safety case prior to the occurrence charter because operations to CYSK are similar to the majority of airports the company services. TC works closely with Perimeter to ensure the company remains compliant with regulatory requirements. A steady flow of information and communication exists. Although TC was aware that the company was operating charter or MEDEVAC flights to CYSK on a frequent basis, it had not required that Perimeter complete a safety case to identify any risk factors associated with operations there prior to the occurrence flight. The purpose of completing a safety case is to evaluate feasibility of conducting a particular charter flight while maintaining a certain level of safety. Although an administrative exercise, the safety case is meant to identify risk factors associated with a destination, and mitigate any existing threats to a reasonable extent. Threats may vary depending on the destination, weather, and time of day; therefore, threats inherent to the type of operation may be foreseeable and manageable. The safety case is part of the company safety management system (SMS), which is overseen by TC.The company had at times seated passengers with limited mobility or those assisting others next to the main door exit as this seat offers the most room to assist and/or manoeuvre. The company's own SMS had not captured this non-compliant practice. If non-compliant practices are not identified, reported, and dealt with by a company's SMS, there is a risk that they will not be addressed in a timely manner.
Process Inspections (PI) conducted by TC at Perimeter prior to the occurrence did not identify the non-compliant practice of seating passengers with limited mobility or those assisting others next to an emergency exit. The likely reason for TC not identifying this hazard is that, at the time the PIs were conducted, the seating of passengers with limited mobility or those assisting others next to emergency exits was not witnessed. PIs are most often related to administrative requirements and proper documentation outlined in the company SMS. If TC's oversight is dependent on the effectiveness of a company's SMS reporting of safety issues, there is a risk that important safety issues will be missed.
Program validation inspections (PVI) and process inspections (PI) are conducted to identify any non-conformity to regulatory requirements; however, they are also meant to identify any hazards that could affect the safety of a flight or that could cause injury or death. The post-occurrence PI did not produce any findings or conclusions regarding the seating of the mother and infant in the exit row, or make any recommendations regarding the safety issue of the non-use of CRS for the infant.
3.0 Findings
3.1 Findings as to causes and contributing factors
- The lack of required flight documents, such as instrument approach charts, compromised thoroughness and placed pressure on the captain to find a work-around solution during flight planning. It also negatively affected the crew's situational awareness during the approaches at CYSK (Sanikiluaq).
- Weather conditions below published landing minima for the approach at the alternate airport CYGW (Kuujjuarapik) and insufficient fuel to make CYGL (La Grande Rivière) eliminated any favourable diversion options. The possibility of a successful landing at CYGW was considered unlikely and put pressure on the crew to land at CYSK (Sanikiluaq).
- Frustration, fatigue, and an increase in workload and stress during the instrument approaches resulted in crew attentional narrowing and a shift away from well-learned, highly practised procedures.
- Due to the lack of an instrument approach for the into-wind runway and the unsuccessful attempts at circling, the crew chose the option of landing with a tailwind, resulting in a steep, unstable approach.
- The final descent was initiated beyond the missed approach point and, combined with the 14-knot tailwind, resulted in the aircraft remaining above the desired 3-degree descent path.
- Neither pilot heard the ground proximity warning system warnings; both were focused on landing the aircraft to the exclusion of other indicators that warranted alternative action.
- During the final approach, the aircraft was unstable in several parameters. This instability contributed to the aircraft being half-way down the runway with excessive speed and altitude.
- The aircraft was not in a position to land and stop within the confines of the runway, and a go-around was initiated from a low-energy landing regime.
- The captain possibly eased off on the control column in the climb due to the low airspeed. This, in combination with the configuration change at a critical phase of flight, as called for in the company procedures, may have contributed to the aircraft's poor climb performance.
- A rate of climb sufficient to ensure clearance from obstacles was not established, and the aircraft collided with terrain.
- The infant passenger was not restrained in a child restraint system, nor was one required by regulations. The infant was ejected from the mother's arms during the impact sequence, and contact with the interior surfaces of the aircraft contributed to the fatal injuries.
3.2 Findings as to risk
- If instrument approaches are conducted without reference to an approach chart, there is a risk of weakened situational awareness and of error in following required procedures, possibly resulting in the loss of obstacle clearance and an accident.
- If additional contingency fuel is not accounted for in the aircraft weight, there is a risk that the aircraft may not be operated in accordance with its certificate of airworthiness or may not meet the certified performance criteria.
- If Transport Canada crew resource management (CRM) training requirements do not reflect advances in CRM training, such as threat and error management and assertiveness training, there is an increased risk that crews will not effectively employ CRM to assess conditions and make appropriate decisions in critical situations.
- If a person assisting another is seated next to an emergency exit, there is an increased risk that the use of the exit will be hindered during an evacuation.
- If a person holding an infant is seated in a row with no seat back in front of them, there is an increased risk of injury to the infant as no recommended brace position is available.
- If young children are not adequately restrained, there is a risk that injuries sustained will be more severe.
- If a lap-held infant is ejected from its guardian's arms, there is an increased risk the infant may be injured, or cause injury or death to other occupants.
- If more complete data on the number of infants and children travelling by air are not available, there is a risk that their exposure to injury or death in the event of turbulence or a survivable accident will not be adequately assessed and mitigated.
- If temperature corrections are not applied to all altitudes on the approach chart, there is an increased risk of controlled flight into terrain due to a reduction of obstacle clearance.
- If the missed approach point on non-precision instrument approaches is located beyond the 3-degree descent path, there is an increased risk that a landing attempt will result in a steep, unstable descent, and possible approach-and-landing accident.
- If there is not sufficient guidance in the standard operating procedures, there is a risk that crews will not react and perform the required actions in the event that ground proximity warning system warnings are generated.
- If standard operating procedures, the Airplane Flight Manual and training are not aligned with respect to low-energy go-arounds, there is a risk that crews may perform inappropriate actions at a critical phase of flight.
- If non-compliant practices are not identified, reported, and dealt with by a company's safety management system, there is a risk that they will not be addressed in a timely manner.
- If Transport Canada's oversight is dependent on the effectiveness of a company's safety management system's reporting of safety issues, there is a risk that important issues will be missed.
3.3 Other findings
- The quick response of the people on the ground reduced the exposure of passengers and crew to the elements.
4.0 Safety action
4.1 Safety action taken
4.1.1 Perimeter Aviation LP
4.1.1.1 Operational planning issues
Various dispatch/operations functions are now centralized in a systems operations control centre (SOCC) at the Winnipeg (CYWG) main base. The Flight Dispatch Centre, Winnipeg YWG Ops, Thompson YTH Ops, MEDEVAC Dispatch, and Charter Coordination are under one roof, communicating and sharing information with each other. Specific procedures have been developed for communicating (over the radio) to the various operational units. Although the 703/704 and 705 program are authorized in the company operations manual (COM) as separate operational control functions, operations conducted under Subpart 703 and 704 benefit from all the advantages of the Type B dispatcher flow since the creation of the SOCC.4.1.1.2 Resource management
To address concerns with resource management, Perimeter enhanced the procedure whereby flight crews access the Canada Air Pilot (CAP) instrument approach charts by increasing the subscription numbers and locations (Canada and United States) to the CAP, and by making them accessible in the SOCC, 24 hours a day, 7 days a week. An electronic version of the charts is now available to flight crews on the company intranet site.Route/charter packages have been developed and populated on the company intranet site to further enhance communication and resources available to the flight crews when conducting charter flights. The charters checklist has been improved to enhance communication on what is required for any given trip and where to retrieve the required items.
4.1.1.3 Passenger briefings
In March 2013, Perimeter changed its passenger briefings procedure in order to ensure uniformity in the briefing delivered. Passenger briefing Q-cards were produced and placed in each aircraft. The first officer now reads the briefing verbatim from this card to ensure that all items are covered. A first review of the new briefing was completed in June 2013. Auditing of this new briefing content and conduct was executed through the company safety management system (SMS). Employee feedback has been positive. Passenger briefings are now part of the annual pilot proficiency check.4.1.1.4 Stabilized approach
In December 2013, Perimeter added a Stabilized Approach section to the Metro II and Metro III standard operating procedures. This section defines the conditions for a stabilized approach for a visual flight rules arrival and an instrument flight rules arrival. Stabilized approach criteria are detailed. Any deviation from a stabilized approach profile must result in a missed approach.4.1.1.5 Stabilized constant descent angle approaches
In December 2013, Metro II and Metro III SOPs were modified to include a section defining stabilized constant descent angle non-precision approaches criteria and its use in flight operations.4.1.1.6 Ground proximity warning system training
In August 2013, Perimeter introduced a more detailed version of the ground proximity warning system (GPWS) training in order to highlight the operating features and parameters of the system. This will increase flight crews' understanding of the various warnings provided, and the necessary actions to be taken when these warnings are activated.In December 2013, SOPs applicable to the Metro II and Metro III were modified to include each of the GPWS warnings, and associated mandatory action. The training department has put emphasis on the importance of the stabilized go-around procedure and its sequential steps.
4.1.1.7 Standard calls for go-around (crew coordination)
In December 2013, the SOPs were revised to emphasize the roles of the pilot flying and pilot not flying (crew coordination) and standardized phraseology to be used during the go-around procedure for a missed approach, balked landing or when encountering windshear. The go-around procedure was changed so as to wait for a positive rate of climb and prior to retracting gear and raising flaps to the ½ position. Better definition of flight parameters was provided to help crews with the go-around decision-making process and improve the execution of go-around procedures.4.1.1.8 Charter packages
Since the accident, Perimeter has produced charter packages for charter flights. These are similar to those prepared for scheduled routes.4.1.1.9 Crew resource management training
In 2013, Perimeter used reports from its own SMS for the first time to build more realistic examples of crew interactions, and also used crew input. Feedback on this crew resource management training approach was positive.4.2 Safety action required
4.2.1 Reporting of number of infant and child passengers travelling by air
According to the International Civil Aviation Organization, in 2013, the number of passengers carried rose to 3.1 billion, which i 4.5% higher than for 2012.Footnote 124 In terms of domestic scheduled air services, all regions experienced an increase in traffic, and markets overall grew by 5.1% in 2013. North America is still the world's largest domestic market with 45% of the world domestic scheduled traffic. There are no statistics on the number of infants and children travelling.Transport Canada statistics show that passenger traffic at Canadian airports increased 2.9% in 013, to reach 85.2 million enplaned and deplaned passengers. Domestic, Canada–U.S., and other international traffic increased year-over-year by 2.8%, 4.4%, and 1.6%, respectively.Footnote 125 The number of infants and child passengers travelling by air is not available.
Currently, under the Transportation Information Regulations, Canadian air carriers must provide a wide range of information on their overall operations to the Minister of Transport. However, information on the number of infant and child passengers travelling is not required to be reported. Historical information supplied by Perimeter and 3 other air carriers in the course of this investigation indicated that infants 0 to 2 years old and children 2 to 12 years old made up nearly 14% of their total passenger loads.
Data relevant to the number of infants may be available but not stored for easy retrieval, and the number of children (under 12 years old) travelling is contained within the number of passengers. As a result, the exact number of infants and young children travelling on board an aircraft, and whether or not infants are carried on a guardian's lap or in a separate seat, is not available and makes it difficult to properly assess infant and child passenger exposure to air travel.
Until better data collection is required, the industry will be unable to conduct research, assess risks, and outline emerging trends related to the carriage of infants and children. If more complete data on the number of infants and children travelling are not available, there is a risk that their exposure to injury or death in the event of in-flight turbulence or a survivable accident will not be adequately assessed and mitigated.
Therefore, the Board recommends that:
The Department of Transport require commercial air carriers to collect and report, on a routine basis, the number of infants (under 2 years old), including lap-held, and young children (2 to 12 years old) travelling.TSB Recommendation A15-01
4.2.2 Required use of child restraint systems
Although there is a lack of data readily available on the number of infants and child passengers travelling, data retrieved from a sample of 4 Canadian operators in the course of this investigation show that children and infants make up a significant portion (nearly 14%) of their total passengers. These numbers reflect only a portion of the number of infants and children travelling by air. There are currently 583 registered commercial fixed-wing operators in Canada. TC statistics show that passenger traffic at Canadian airports increased 2.9% in 2013, to reach 85.2 million enplaned and deplaned passengers.Biomechanical research has found that, due to limitations in human clasping strength, it is not always possible for adults to restrain children adequately in their laps by holding onto them. Infants are therefore exposed to undue risk of injury when seated on an adult's lap. In most countries around the world, including Canada, infants are not required to be restrained in an age- and size-appropriate child restraint system (CRS) at any time during a flight. Research has also shown that, given the specific physical features of young children, the standard adult seatbelt does not provide a suitable method of restraint.
Most jurisdictions recommend that infants and young children travel restrained in an approved CRS during a flight; however, its use is not mandatory. Although research has been conducted over the last 25 years, and participation in the development of CRS standards and training standards has taken place and is ongoing, there has been no progress on the required use of appropriate CRS on commercial aircraft.
Although passengers are required to securely stow all carry-on baggage during takeoff and landing because of the potential risk of injury to other passengers should an unexpected hazardous event occur, passengers continue to be permitted to hold in their lap a child of a size and weight equal to carry-on baggage. If children under 2 years old are not required to be restrained for their own safety, the safety of other passengers also becomes an issue.Footnote 126
The National Transportation Safety Board of the United States has identified several occurrences where crew, adult passengers, and children have sustained injury during unexpected moderate-to-severe turbulence, and described how lap-held infants and children would likely have survived the occurrences or suffered less severe injury had they been properly restrained.Footnote 127 A number of aircraft accidents, including the occurrence under investigation, have demonstrated the risk to infants and young children who are not properly restrained. Given the overall safety performance of commercial aviation, passengers may underestimate the risks associated with unexpected in-flight turbulence and emergency situations.
TC has no further plans to educate the travelling public or promote the use of CRS at this time. The Board is concerned that until such time as the use of age- and size-appropriate CRS is required, parents and guardians will continue to travel with infants and children without the safety benefits provided by CRS.
Infants and children who are not properly restrained are at risk of injury and possibly death, and may cause injury or death to other passengers. Until new regulations on the use of CRS are implemented, lap-held infants and young children are exposed to undue risk and are not provided with an equivalent level of safety compared to adult passengers.
Therefore, the Board recommends that:
The Department of Transport work with industry to develop age- and size-appropriate child restraint systems for infants and young children travelling on commercial aircraft, and mandate their use to provide an equivalent level of safety compared to adults.This report concludes the Transportation Safety Board's investigation into this occurrence. The Board authorized the release of this report on 10 June 2015. It was officially released on 29 June 2015.TSB Recommendation A15-02
Appendices
Appendix A – Sanikiluaq, NU, NDB RWY 27 (GNSS)
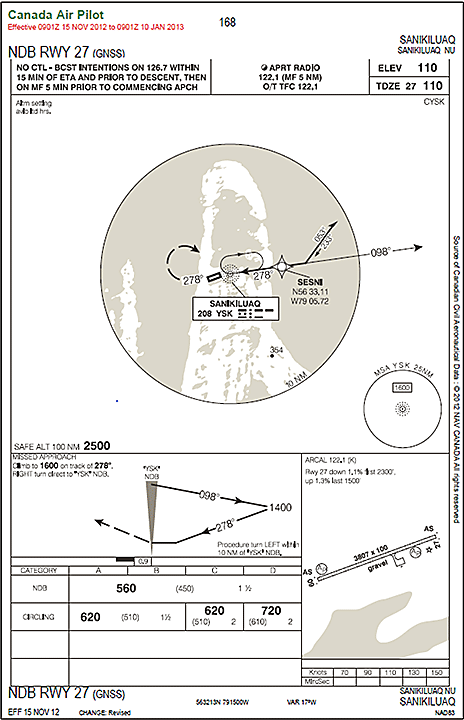
NOT FOR NAVIGATION
Appendix B – Flight path
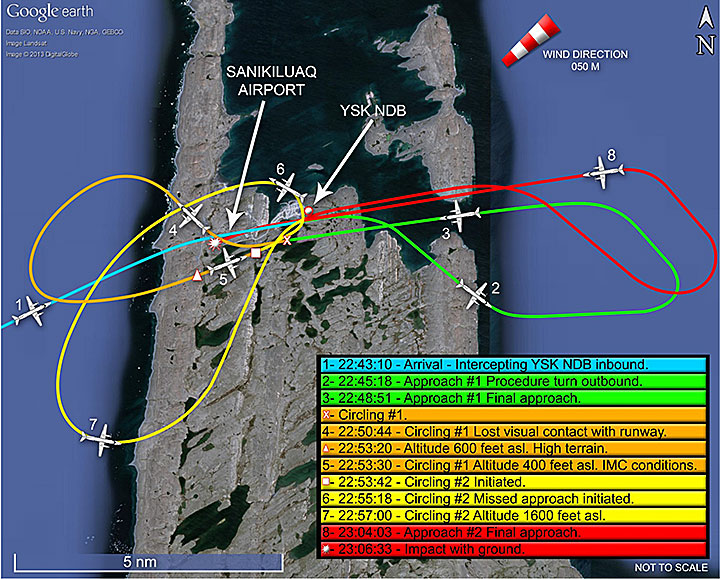
Appendix C – Sanikiluaq, NU (CYSK) aerodrome chart
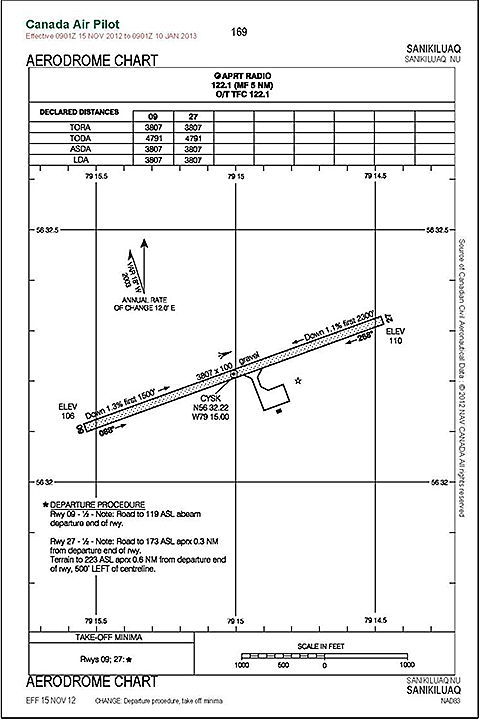
NOT FOR NAVIGATION
Appendix D – Flight path profile
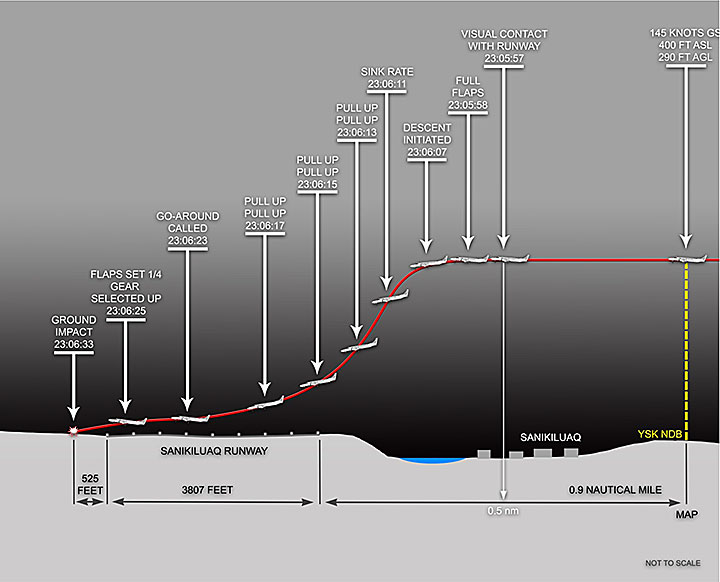
Appendix E – Graphic area forecast (GFA)
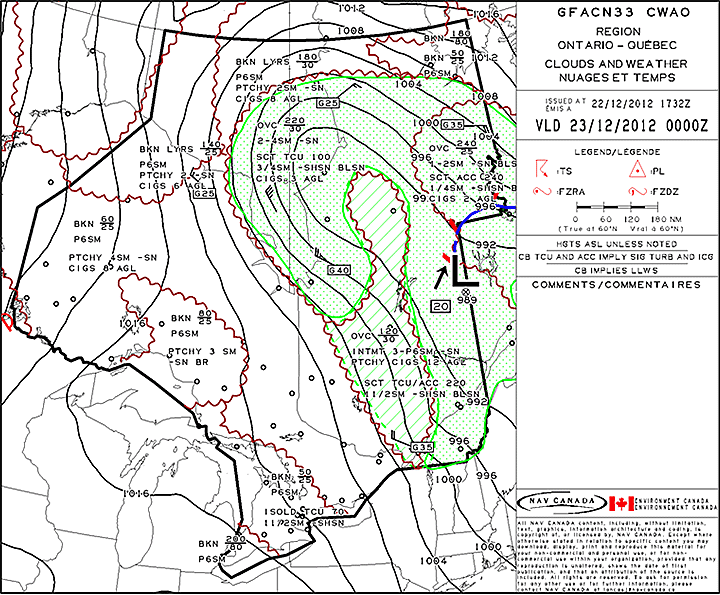
Appendix F – International policy and efforts regarding child restraint systems and in-flight safety
International policies regarding the use of child restraint systems
Many jurisdictions (e.g., European Union, Australia, New Zealand) permit, or even require, lap-held infants to be restrained with a supplementary or a belly loop belt, which attaches to the adult's seatbelt and goes around the infant's abdomen. Canada and the United States do not allow the supplementary loop belt because research has shown that infants so restrained fare worse than unrestrained infants because of the adult's forward movement during severe impact and the concentrated forces of the supplementary loop belt on the infant's abdominal region.Footnote 128A 2004 Australian study found that, although the infant anthropomorphic dummy attached with a supplementary loop belt was restrained during dynamic testing, it underwent significant forward excursion resulting in severe impact of the infant dummy's head with the forward seat back. In addition, the adult dummy folded over the infant dummy trapping and crushing it in the process.Footnote 129 A comprehensive reviewFootnote 130 of the scientific literature on child restraint systems (CRS) in aviation, specifically that addressing the protection from injuries in survivable aviation occurrences for children under 2 years old, as well as accident reports, concluded that in order to provide safety equivalent to that of adult passengers, infants “should be seated in a suitable CRS on a seat of their own.” The report authors further conclude that, “the transport of lap-held infants secured with or without a loop belt does not provide any protection to the infant.”
Previous recommendations for child restraint systems
National Transportation Safety Board
The National Transportation Safety Board (NTSB) has issued several recommendationsFootnote 131 on the subject of the mandatory use of CRS for infant passengers, the appropriate use of safety harnesses for children, and educating the public on the risks associated with not using a CRS for children under the age of 2.The NTSB's Child and Youth Transportation Safety Initiative promotes child occupant safety in all modes of transportation with a focus on educating parents and caregivers about ways to keep children safe when travelling. The NTSB declared 2011 the Year of the Child and initiated a study on children involved in general aviation (GA) accidents and incidents. During 2011, the NTSB collected data on 19 GA accidents and incidents, which included 39 children who were 14 years old and younger. In total, 26 children sustained fatal injuries, 2 sustained serious injuries, 5 sustained minor injuries, and 6 sustained no injuries. All of the children under 2 years old were restrained in a CRS and sustained no injuries in the accidents.Footnote 132
The NTSB has also put forward the argument that, although passengers are required to securely stow all carry-on baggage during takeoff and landing because of the potential risk of injury to other passengers in the event of an unexpected hazardous event, passengers continue to be permitted to hold a child of equal size and weight in their lap. When children under the age of 2 are not required to be restrained for their own safety, the safety of other passengers also becomes an issue.Footnote 133
Additionally, the NTSB has highlighted several occurrences where crew, passengers and children have sustained injury during unexpected moderate-to-severe turbulence and described how lap-held infants and children would have likely survived the occurrences or suffered less severe injury had they been properly restrained.Footnote 134
The most recent sudden in-flight turbulence event happened on 17 February 2014, when a Boeing 737-700 encountered sudden severe turbulence while on descent to land in Billings, Montana. A flight attendant was critically injured. A lap-held infant flew out of its mother's arms to land in an empty seat 2 rows away; the infant was not injured. A total of 3 flight attendants and 2 passengers were taken to hospital.
European Aviation Safety Agency
The European Aviation Safety Agency (EASA) conducted a study on CRS in 2007.Footnote 135 Phase II of the study, involving the evaluation of available solutions for restraining infants and children, states that the standard lap belt is not suited for a safe restraint of infants/children. The iliac crest of infants/children is not yet fully developed and, therefore, there is a danger that the lap belt will slip into the infant/child abdominal region in an accident or turbulence, resulting in severe internal injuries. In addition, tests revealed that in the dynamics of a crash, the upper torso of an infant/child can hit against the femurs. The head can hit against the seat in front or the structure of its own seat. The study concludes by stating that:Child seats must be adapted to the infant /child development in order to provide safe restraint. Child Restraint DeviceFootnote 136 requirements must include (in part):
- Infants up to a weight of approx. 9 kg must be transported backward-facing in a CRS.
- Forward-facing CRD must be equipped with restraint systems which are appropriate for children, i. e. either with a belt restraint system or with an impact shield. A belt restraint system which is appropriate for children restrains the pelvis and the upper torso safely in an accident and is adaptable to the infant's / child's size. In an impact shield system, the infant's / child's pelvis and thorax (sternum) are supported by the impact shield.
- The belt restraint system of forward-facing CRD must be equipped with an additional crotch belt preventing the infant/child from slipping under the lap belt.
Safety efforts pertaining to in-flight turbulence
Transport Canada
In-flight turbulence is the leading cause of injuries to passengers and flight attendants. There have been several accidents and incidents over the years involving clear air turbulence that highlight the importance of keeping loose objects restrained and safety belts fastened throughout a flight. In January 2012, Transport Canada (TC) issued Advisory Circular (AC) 605-004, Issue No. 1 – Use of Safety Belts by Passengers and Crew Members, in order to emphasize the importance of using the proper restraints during all phases of flight, as sudden, moderate-to-severe turbulence can be the cause of injuries to all on board. It also states that lap-held infants remain subject to injury if not secured during periods of turbulence.Federal Aviation Administration
In 1995, after several serious and unexpected events of turbulence, the Federal Aviation Administration (FAA) issued a public advisory to airlines urging the use of seatbelts at all times when passengers are seated. Most airlines now comply, but the requirement does not apply to children younger than 2 years because they are not required to be restrained at any time during the flight.Following several occurrences involving fatalities and/or injuries during moderate-to-severe turbulence in flight, the FAA issued an Advisory CircularFootnote 137 in 2006 addressing the subject of Preventing Injuries Caused by Turbulence. The AC provided information and practices that were known to be effective in preventing injuries caused by turbulence, which includes prompt and clear communication between flight crew and flight attendants, and with passengers on staying seated with seatbelts fastened. It also stressed the importance for flight attendants to secure the cabin equipment so that loose objects will not be thrown about the cabin. The AC also suggested that air carriers develop and implement practices to encourage the use of an approved CRS to secure an infant or a small child that is appropriate for that child's size and weight; regulations on CRS, however, have not changed. The AC states:
Parents and guardians should be encouraged to have children under 2, occupy an approved CRS any time the fasten seatbelt sign is illuminated. Flight attendants are encouraged to verify that the CRS is secured properly in a forward facing seat and that the child appears to be properly secured in the CRS.On 17 September 2010, the FAA issued Advisory Circular AC 120-87B – Use of Child Restraint Systems (CRS) on Aircraft. The AC was intended to be a resource for the development, implementation and revision of air carriers' standard operating procedures and training programs regarding the use of CRS. Although this AC provides considerable information regarding CRS for children over the age of 2, it does not address children under the age of 2. The AC indicates that children under the age of 2 may be held in an adult's lap during takeoff, landing or movement on the surface.
Efforts by the International Civil Aviation Organization
The International Civil Aviation Organization (ICAO) statedFootnote 138 that, in 2013, the number of passengers carried rose to 3.1 billion, which is 4.5% higher than for 2012.In terms of domestic scheduled air services, all regions experienced an increase in traffic, and markets overall grew by 5.1% in 2013. North America is still the world's largest domestic market with 45% of the world domestic scheduled traffic. There are no statistics on the number of infants and children travelling.
Transport Canada (TC) statistics show that passenger traffic at Canadian airports increased 2.9% in 2013, to reach 85.2 million enplaned and deplaned passengers. Domestic, Canada–U.S. and other international traffic increased year-over-year by 2.8%, 4.4%, and 1.6%, respectively.Footnote 139 These statistics are in line with those reported by ICAO. The number of infants and children passengers travelling by air is not available.
The issue of child safety restraints was recently raised by ICAO member states. ICAO was asked to lead the states on how to best approach the issue. The issue of child safety restraints is included in the 2014-2016 triennium work program for the assigned ICAO Cabin Safety Group (ICSG). The group is composed of 28 participants from various member states, representing various international groups, such as airlines, regulators (including TC), flight attendant respresentatives, and aircraft manufacturers. The working group met in April 2014 to pursue work on the development of guidance on the safety of infants and the use of child restraint systems.Footnote 140
The International Transport Workers' Federation presented a working paper to ICAO for the Assembly – 38th Session Technical Commission, addressing the child restraint issue. The Executive Summary states:
One of the goals of aviation safety is that all reasonable steps be taken to ensure safe air travel for the flying public and crew members. Cabin crew are responsible for the safety, health and security of all occupants in the cabin of commercial airplanes. While fairness dictates that all passengers be afforded the same level of protection, in many countries the youngest and most vulnerable may be allowed to travel on the lap of an adult for taxi, take-off, landing, and during periods of turbulence, if they are under a certain age. In order to ensure that these youngest passengers remain secured during critical phases of flight and turbulence, the exception to international aviation regulations that allows children to travel in the laps of adults must be eliminated.Footnote 141
Appendix G – Perimeter Metro III go-around procedure
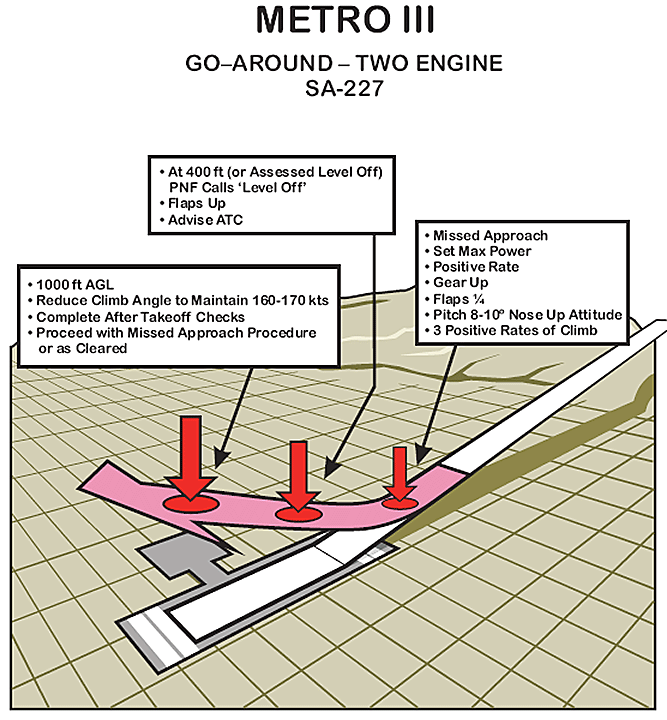
Appendix H – Approach-and-Landing Accident Reduction Task Force recommendations
Recommendations concerning company policies
- Operators should specify well-definedFootnote 142 approach gates.
- Operators should define the parameters of a stabilized approach in their company flight operations manuals (FOM) and aircraft operating manuals (AOM).
- The stabilized approach policy should at least cover the flight path, speed, power setting, altitude and rate of descent, as well as configuration and flight crew landing readiness.
- All flights should be stabilized by 1000 feet agl [above ground level] in IMC [instrument meteorological conditions] and by 500 feet agl in VMC [visual meteorological conditions].
- Operators should develop and support “no-fault” go-around and missed approach policies.
- FOMs or SOPs [standard operating procedures] should require a go-around if an aircraft becomes unstable during approach.
- Operators should implement SCDA [stabilized constant descent angle] procedures for non-precision approaches.
- Operators should develop and implement a policy on appropriate autopilot use in conditions of reduced visibility, at night or in the presence of optical or physiological illusions.
- Operators should establish clear directives for TAWS [terrain awareness warning system] alerts.
Recommendations concerning standard operating procedures
- States should mandate, and operators should develop and implement, SOPs for approach-and-landing operations.
- States should mandate the use of SOPs for approach-and-landing operations.
- Operators should develop SOPs for autopilot use during approaches and landings.
- Operators should have a clear policy on the role of the pilot-in-command in complex situations and train accordingly.
- A risk assessment checklist should be used to identify approach and landing hazards.
Recommendations concerning training
- Crews should be trained to identify operational risks associated with adverse conditions, such as reduced visibility, visual illusions, contaminated runways and cross-winds.
- The training should deal with non-precision approaches, especially those that involve shallow approach paths or stepped descents.
- Crews should be trained to take the time to implement corrective actions when the cockpit situation becomes confusing, ambiguous or task saturated.
- Operators should develop and implement a policy on appropriate autopilot use along with navigation aids for the approaches being flown.
- Crews should receive training on SCDA approach procedures.
- Crews should be educated about approach design criteria and minimum obstacle clearance requirements.
Recommendations concerning decision making
- Operators should provide education and training that enhance decision making and risk (error) management.
- Operators should develop a decision-making model for use in time-critical situations (where the time available for decision making is limited).
- Operators should provide improved training on error management and risk assessment as well as on mitigating the consequences of errors.
Recommendations concerning cockpit voice recorders and flight data recorders
- Regulatory authorities should encourage the installation of FDRs [flight data recorder] and CVRs [cockpit voice recorder] on aircraft for which they are currently not required.
Recommendations concerning autopilot
- The FSF [Flight Safety Foundation] Task Force recommended that the autopilot be used, especially in conditions of reduced visibility, at night or in the presence of optical or physiological illusions.
Recommendations concerning radio altimeter
- Operators should state that the radio altimeter is to be used during approach operations and specify procedures for its use.
- Train crews to correct the radio altimeter bug to 200 feet agl on all approaches except for CAT [Category] II and III.
- Train crews to initiate an aggressive go-around if the alarm sounds without visual contact being established with the runway.
- Operators should activate automatic callouts or require callouts from their crews, at 2500, 1000 and 500 feet agl as well as at the minimums.
Recommendations concerning the stabilized constant descent angle approach technique
- Implement use of SCDA procedure for non-precision approaches.
- Crews should receive training on SCDA approach procedures.
- Crews should be educated on approach design criteria and minimum obstacle clearance requirements.
Appendix I – List of acronyms and abbreviations
- AC
- Advisory Circular
- AFM
- Airplane Flight Manual
- agl
- above ground level
- AIM
- Aeronautical Information Manual
- ALA
- approach-and-landing accident
- ALAR
- Approach-and-Landing Accident Reduction (FSF task force)
- AMO
- approved maintenance organization
- AOC
- Air Operator's Certificate
- AOM
- aircraft operating manual
- APAPI
- abbreviated precision approach path indicator
- ARCAL
- Aircraft Radio Control of Aerodrome Lighting
- ARFF
- aircraft rescue and fire fighting
- asl
- above sea level
- ATC
- air traffic control
- ATIS
- automatic terminal information service
- ATPL
- airline transport pilot licence
- C
- Celsius (degrees)
- CAA
- Civil Aviation Authority (United Kingdom)
- CAD
- Canadian Aviation Document
- CAM
- cockpit area microphone
- CAO
- Civil Aviation Order
- CAP
- Canada Air Pilot
- CAP GEN
- Canada Air Pilot General Pages
- CARAC
- Canadian Aviation Regulation Advisory Council
- CARC
- Civil Aviation Regulatory Committee (part of CARAC)
- CARs
- Canadian Aviation Regulations
- CARS
- community aerodrome radio station
- CASA
- Civil Aviation Safety Authority (Australia)
- CASS
- Commercial Air Service Standards
- CFIT
- controlled flight into terrain
- CFS
- Canada Flight Supplement
- COM
- Company Operations Manual
- CPL
- commercial pilot licence
- CRD
- child restraint device
- CRM
- crew resource management
- CRS
- child restraint system
- CVR
- cockpit voice recorder
- CYBR
- Brandon
- CYDN
- Dauphin
- CYGL
- La Grande Rivière
- CYGW
- Kuujjuarapik
- CYMO
- Moosonee
- CYPL
- Pickle Lake
- CYQK
- Kenora
- CYSK
- Sanikiluaq
- CYWG
- Winnipeg/James Armstrong Richardson International Airport
- DA(H)
- decision altitude/height
- DH
- decision height
- EASA
- European Aviation Safety Agency
- EGT
- exhaust gas temperature
- EIC
- Exchange Income Corporation
- FAA
- Federal Aviation Administration (United States)
- FDR
- flight data recorder
- FIC
- flight information centre
- FO
- first officer
- FOM
- flight operations manual
- FOQA
- Flight Operational Quality Assurance
- ft/min
- feet per minute
- FSF
- Flight Safety Foundation
- FTM
- Flight Training Manual
- g
- gravitational acceleration
- GA
- general aviation
- GFA
- graphic area forecast
- GNSS
- global navigation satellite system (approach)
- GPS
- global positioning system
- GPWS
- ground proximity warning system
- IAS
- indicated airspeed
- IATA
- International Air Transport Association
- ICAO
- International Civil Aviation Organization
- ICSG
- ICAO Cabin Safety Group
- IFR
- instrument flight rules
- ILS
- instrument landing system
- IMC
- instrument meteorological conditions
- in. Hg
- inches of mercury
- ISA
- international standard atmosphere
- kg
- kilogram
- KIAS
- knots indicated airspeed
- LOSA
- Line Operations Safety Audit
- LPV
- Localizer Performance with Vertical Guidance
- M
- Magnetic (degrees)
- MAC
- Manitoba Aviation Council
- MANAIR
- Manual of Standards and Procedures for Aviation Weather Forecasts
- MAP
- missed approach point
- MCTOW
- maximum certificated take-off weight
- MDA
- minimum descent altitude
- MDA (H)
- minimum descent altitude/height
- MEDEVAC
- medical evacuation
- MEL
- Minimum Equipment List
- MEL/CDL
- minimum equipment list / configuration deviation list
- METAR
- aviation routine weather report
- MHz
- megahertz
- MSA
- minimum safe altitude
- NATA
- Northern Air Transport Association
- NDB
- non-directional beacon
- NDB RWY 27 (GNSS)
- non-directional beacon Runway 27 global navigation satellite system (approach)
- nm
- nautical mile
- NOTAM
- Notice to Airmen
- NPA
- non-precision approach
- NTSB
- National Transportation Safety Board (United States)
- OFP
- operational flight plan
- OpSpec/OPS Spec
- Operations Specification
- PAG
- Perimeter charter flight PAG 993
- PAPI
- precision approach patch indicator
- PDM
- Pilot Decision Making
- PE
- Pilot Examiner
- Perimeter
- Perimeter Aviation LP
- PF
- pilot flying
- PI
- Process Inspection
- PIC
- pilot-in-command
- PMA
- pilot monitored approach
- PNF
- pilot not flying
- PVI
- Program Validation Inspection
- QAP
- quality assurance program
- RA/TA
- resolution advisory / traffic advisory
- RCMP
- Royal Canadian Mounted Police
- REM
- rapid eye movement (sleep)
- RNAV
- area navigation (approach)
- RSC
- runway surface condition
- SCDA
- stabilized constant descent angle
- sm
- statute mile
- SMS
- safety management system
- SOCC
- Systems Operations Control Centre
- SOP
- standard operating procedures
- SPPA
- Standard Project Planning Application
- SRL
- Single Redline Limit
- STEADES
- Safety Trend Evaluation, Analysis & Data Exchange System (IATA system)
- T
- True (degrees)
- TAF
- aerodrome forecast
- TAWS
- terrain awareness and warning system
- TC
- Transport Canada
- TCAS
- traffic alert and collision avoidance system
- TCCA
- Transport Canada Civil Aviation
- TCU
- towering cumulus (cloud)
- TEM
- threat and error management
- TSB
- Transportation Safety Board of Canada
- TSO
- Technical Standard Order (issued by the FAA)
- U/S
- unserviceable
- UTC
- Coordinated Universal Time (Central Standard Time plus 6 hours; Eastern Standard Time plus 5 hours)
- VASIS
- visual approach slope indicator system
- VFR
- visual flight rules
- VHF
- very high frequency
- VMC
- visual meteorological conditions
- VREF
- reference speed
- VYSE
- one engine inoperative best rate-of-climb speed
- YSK
- 3-letter identifier for the Sanikiluaq non-directional beacon
Footnotes
- Footnote 1
-
The SA227-AC is also known as the Metro III or the SW4.
- Footnote 2
-
Please refer to Appendix I – List of acronyms and abbreviations.
- Footnote 3
-
Commuter air transport service (i.e. a multi-engine aeroplane) that
has a maximum certificated take-off weight (MCTOW) of 8618 kg (19 000
pounds) or less and a seating configuration, excluding pilot seats, of
10 to 19 seats.
- Footnote 4
-
Perimeter Aviation LP falls under the umbrella of Exchange Income
Corporation (EIC). Other related companies that fall under EIC are Calm
Air, Bearskin Airlines, Keewatin Air, Custom Helicopters, and Regional
One.
- Footnote 5
-
All times Coordinated Universal Time (UTC) (Central Standard Time
plus 6 hours; Eastern Standard Time plus 5 hours). UTC is used in this
report due to multiple time zones.
- Footnote 6
-
Alternate aerodrome means an aerodrome to which a flight may proceed
when landing at the intended aerodrome of destination becomes
inadvisable.
- Footnote 7
-
Perimeter Aviation LP, Company Operations Manual (COM),
Section 17.3.11 requires that a survival kit be on board when the flight
takes place above 66° latitude in uncontrolled airspace or off
designated routes. However, due to its remote location and environment,
Sanikiluaq is an exception (survival kit required) despite being located
south of 66° latitude.
- Footnote 8
-
Perimeter Aviation LP, Company Operations Manual (COM), Section 10.8.9, Individual Safety Briefing, and Canadian Aviation Regulations (CAR) 724.34 (2).
- Footnote 9
-
Flight Level 230, 23 000 feet above mean sea level.
- Footnote 10
-
Canadian Aviation Regulations (CAR) 602.88 (4) (a) and 704.20 (a) Fuel requirements for a flight conducted under IFR [instrument flight rules].
- Footnote 11
-
Perimeter Aviation LP, Company Operations Manual (COM), Chapter 9, Section 9.15.2.5 Gravel Runway Operations (704), (Ops Spec 029).
- Footnote 12
-
VREF (reference speed) is 1.3 times the stall speed with
full landing flaps or with selected landing flaps. Speed calculated to
cross threshold.
- Footnote 13
-
All speeds are indicated airspeed (IAS) unless otherwise specified.
- Footnote 14
-
Indicated altitude shows altitude above sea level (asl) and is read
directly from the altimeter when set to the current barometric pressure.
- Footnote 15
-
The minimum descent altitude (MDA) is a specified altitude
referenced to sea level for a non-precision approach below which descent
must not be made unless the visual reference required to continue the
approach to land has been established.
- Footnote 16
-
Circling is an instrument flight rules (IFR) procedure that is
conducted by visually manoeuvring an aircraft, after completing an
instrument approach to one runway, into position for landing on another
runway. Visual contact with the runway environment must be maintained
during the circling manoeuvre. The minimum descent altitude (MDA)
provides 300 feet above all obstacles within the visual manoeuvring
area.
- Footnote 17
-
Go-around - a transition from an approach to a stabilized climb.
- Footnote 18
-
400 feet above sea level (asl) – 223 feet terrain height = 177 feet
above ground level (agl). Application of cold temperature corrections,
the true altitude above ground was 155 feet agl. Terrain information is
also available in the Canada Flight Supplement.
- Footnote 19
-
The published missed approach procedure for the CYSK NDB Runway 27
dictates a climb to 1600 feet on a track of 278°, then return to the YSK
NDB.
- Footnote 20
-
Fairchild, SA227-AC Airplane Flight Manual, Section 4B-17 8AC.
- Footnote 21
-
GNSS: stands for global navigation satellite system, and is the
standard generic term for satellite navigation systems that provide
autonomous geo-spatial positioning with global coverage, e.g. GPS
navigation.
- Footnote 22
-
Canadian Aviation Regulations (CAR) 602.128 (2) (b) “…no
pilot-in-command of an IFR aircraft shall, in the case of a
non-precision approach, descend below the minimum descent altitude,
unless the required visual reference necessary to continue the approach
to land has been established.”
- Footnote 23
-
The SA227 Perimeter Standard Operating Procedures target
climb speed is 140 knots. However, the average target climb speed for
the Metro III, depending on the weight of the aircraft but for most
weights, is approximately 110 knots.
- Footnote 24
-
Canadian Aviation Regulations (CAR) 700.16 and Perimeter Aviation LP, Company Operations Manual,
Chapter 8, Section 8.6.7: The maximum flight duty time allowed for the
flight crew member, operating under Subpart 704 operations, is normally
14 consecutive hours in any 24 consecutive hours. The maximum flight
time and flight duty time may be exceeded by 3 consecutive hours if the
flight is extended as a result of “unforeseen operational circumstances”.
If less than 9 seats had been made available, the return flight could
have been conducted under Subpart 703 operations, in which case maximum
flight duty time is 15 hours in any 24 consecutive hours.
- Footnote 25
-
Subpart 704 (Commercial Air Service) flight operations do not
require that autopilot be installed and used when operated with
2 pilots.
- Footnote 26
-
Perimeter SA-227 Minimum Equipment List, Amendment 2, 31 December 2011, ATA 77-02-1.
- Footnote 27
-
Transport Canada, Aeronautical Information Manual, Section RAC 9.17.1, p. 283.
- Footnote 28
-
Decision height is the height of the decision altitude above the
touchdown zone elevation or runway threshold. The decision altitude is
an altitude specified on a precision approach procedure or an approach
procedure with vertical guidance at which the missed approach procedure
shall be initiated if the visual reference required to continue the
approach to land has not been established. NAV CANADA CAP GEN, Canada Air Pilot, Instrument Procedures, p. 9.
- Footnote 29
-
Transport Canada, Advisory Circular (AC) 600-003, Regulations for Terrain Awareness Warning Systems.
- Footnote 30
-
Honeywell Aerospace, part number 965-0686-001.
- Footnote 31
-
Federal Aviation Administration (FAA), TSO-C129, dated 12/10/92-Airborne Supplemental Navigation Equipment Using the Global Positioning System (GPS).
- Footnote 32
-
Operations Specification, Part IV, No. 100, IFR Instrument Approaches – Global Positioning System (GPS).
- Footnote 33
-
According to the Manual of Standards and Procedures for Aviation Weather Forecasts (MANAIR), Section 2.9.5, the PROB40 of ¾ of a statute mile (sm) would cover visibilities from zero (0) to 1¼ sm.
- Footnote 34
-
Brandon (CYBR) in Manitoba was the chosen alternate airport for the return segment of the charter flight.
- Footnote 35
-
Sanikiluaq (CYSK) is situated in Class G uncontrolled airspace. Air
traffic control has neither the authority nor the responsibility for
exercising control over air traffic. Air Traffic Services units do
provide flight information and alerting services.
- Footnote 36
-
APAPI is an abbreviated precision approach path indicator system
used for aerodromes serving aircraft with eye-to-wheel height of up to
10 feet.
- Footnote 37
-
Leveling of the unit is executed with an inclinometer; at level 0.0,
the angle for Box 2 should be 2 degrees 45 minutes, and at level 0.0,
the angle for Box 1 should be 3 degrees 15 minutes.
- Footnote 38
-
Prevailing visibility is the maximum visibility value common to sectors comprising one-half or more of the horizon circle.
- Footnote 39
-
Observed visibility is the visibility on the ground, taken at eye level.
- Footnote 40
-
Canadian Aviation Regulations (CAR) 605.33 (1).
- Footnote 41
-
Other instruments included the left and right torque gauges, tachometers, fuel flow gauges, and airspeed indicators.
- Footnote 42
-
Pilot Self-Dispatch - means Type C Operational Control where the
pilot-in-command is solely responsible for flight watch but supported by
flight following. The pilot-in-command has the sole authority over the
formulation, execution, and amendment of an operational flight plan
(OFP) in respect of a flight. Commercial Air Service Standards (CASS) 723.16.
- Footnote 43
-
Flight Watch - means maintaining current information on the progress
of the flight and monitoring all factors and conditions that might
affect the OFP [operational flight plan]. Flight Watch begins at brake-release of the aircraft. Perimeter Aviation LP, Company Operations Manual, Section 6.3 Interpretations, p. 6-3.
- Footnote 44
-
Flight Following - means the monitoring of a flight’s progress, the
provision of such operational information as may be requested by the PIC
[pilot-in-command], and the notification of appropriate
Company and search-and-rescue authorities if the flight is overdue or
missing. Perimeter Aviation LP, Company Operations Manual (COM), Section 6.3 Interpretations, p. 6-3.
- Footnote 45
-
Seat identification is indicated as seat 1L = first seat on the left
when looking towards the front of the aircraft, 1R=first seat on the
right, etc. The applicable aircraft certification requirements at the
time of manufacture of the occurrence Metro III required that seats and
their supporting structures be designed to sustain ultimate upward
acceleration loads of 4.5 g, forward acceleration loads of 9.0 g, and
sideward acceleration loads of 1.5 g.
- Footnote 46
-
Canadian Aviation Regulations (CAR) 602.60 (l)(g) requires a
flashlight that is readily available to each crew member, if the
aircraft is operated at night. The crew members carried a flashlight in
their flight bags, but the first officer used what was readily
available.
- Footnote 47
-
Canadian Aviation Regulations (CAR) 704.34, Commercial Air Service Standards (CASS) 724.34(2), and Perimeter Aviation LP, Company Operations Manual,
Chapter 10, Section 10.8.7. The normal safety briefing may be
inadequate if a passenger has physical, sensory or comprehension
limitations, or if a passenger is responsible for another person on
board the aircraft.
- Footnote 48
-
Transport Canada, Commercial and Business Aviation Advisory Circular
No. 0155 (1999). Available at:
http://www.tc.gc.ca/eng/civilaviation/standards/commerce-circulars-ac0155-1633.htm
(last accessed 18 June 2015).
- Footnote 49
-
Commercial Air Service Standards (CASS) 724.35(1)(b)(vii)
Safety Features Card. Available at:
http://www.tc.gc.ca/eng/civilaviation/regserv/cars/part7-standards-724a-2172.htm#724a_35
(last accessed 18 June 2015).
- Footnote 50
-
Flight Safety Foundation, Cabin Crew Safety, “Positions
Brace Passengers for Impact To Reduce Injuries and Fatalities,”
Vol.23(1), January/February 1988. Available at:
http://flightsafety.org/ccs/ccs_jan-feb88.pdf (last accessed
18 June 2015).
- Footnote 51
-
R.F. Chandler, Brace for impact positions. Protection and Survival
Laboratory, p. 5, Civil Aeromedical Institute, Federal Aviation
Administration (FAA): February 1988. Available at:
http://www.unitedafa.org/safety/training/docs/brace.pdf (last accessed
18 June 2015).
- Footnote 52
-
Refers to an impact between a body segment, such as one’s head, and whatever it might hit in a crash.
- Footnote 53
-
Deformable: capable of being reshaped.
- Footnote 54
-
D. Mohan and L.W. Schneider, 1979, “An evaluation of adult clasping
strength for restraining lap-held infants,” Human Factors, 21(6),
pp. 635-645.
- Footnote 55
-
Bill McGee, “Why you should never fly with a child in your lap,” USA Today,
30 July 2008. Available at:
http://usatoday30.usatoday.com/travel/columnist/mcgee/2008-07-29-lap-children_N.htm
(last accessed 18 June 2015).
- Footnote 56
-
R.N. Hardy, 1992, CAA paper 92020: The restraint of infants and young children in aircraft.
- Footnote 57
-
Transport Canada, Advisory Circular (AC) 700-014, Passenger Seating
Requirements and Accessible Air Transportation, Issue 1, 21 August 2009.
Available at: http://www.tc.gc.ca/media/documents/ca-opssvs/700-014.pdf
(last accessed 18 June 2015).
- Footnote 58
-
Canadian Aviation Regulations (CAR) 704.33(1)(d), Apron and cabin safety procedures.
- Footnote 59
-
Perimeter Aviation LP, Company Operations Manual, Section 10.8.4.
- Footnote 60
-
Perimeter SA227 Standard Operating Procedures, Section 5
Operational Notes and Directives, Subsection 5.8 Before Start and
Passenger Briefing. Subpart 704 operations do not require a flight
attendant to be on board.
- Footnote 61
-
Only Subpart 705 air operators are required to have a carry-on baggage control program in accordance with Section 705.42 of the Canadian Aviation Regulations (CARs).
- Footnote 62
-
Canadian Aviation Regulations (CAR) 602.86(1), Carry-on Baggage, Equipment and Cargo.
- Footnote 63
-
Australian Government, Civil Aviation Safety Authority, Carriage of
Infants and Children – A review of Section 13 of Civil Aviation Order
(CAO) 20.16.3, Document DP 1301CS, July 2014.
- Footnote 64
-
The category 2 to 12 years old distinguishes a child from an adult
due to their body development and biomechanical dimensions. The European
Aviation Safety Agency (EASA) study states children under the age of 7.
EASA.2007.C.28, Study on Child Restraint Systems, TÜV Rheinland Kraftfahrt GmbH, Team Aviation, November 2008.
- Footnote 65
-
Federal Aviation Administration (FAA) report DOTIFAAJAM-1 1/3 —
Aviation Child Safety Device Performance Standards Review identified
recommended changes applicable to AS5276/l, and consideration is being
given to these recommendations.
- Footnote 66
-
Federal Aviation Administration (FAA) customer help FAQ site
[online], Does the FAA require children on commercial flights to be in
child restraint systems (CRS)?. Available at:
http://faa.custhelp.com/app/answers/detail/a_id/29/kw/child/session
(last accessed on 18 June 2015.)
- Footnote 67
-
National Transportation Safety Board (NTSB), Analysis of Diversion
to Automobile in Regard to the Disposition of Safety
Recommendation A-95-51, at 1 (03 August 2004).
- Footnote 68
-
National Transportation Safety Board (2010). Safety Recommendations A-10-121 through -123.
- Footnote 69
-
Transport Canada, Advisory Circular 605-003, issue No. 3, Child Restraint Systems, effective 30 October 2013.
- Footnote 70
-
K. Poland and N.M. Marshall, A Study of General Aviation Accidents Involving Children in 2011, National Transportation Safety Board, Washington, D.C., United States.
- Footnote 71
-
TSB aviation occurrence number A07P0369.
- Footnote 72
-
Transportation Information Regulations (SOR/96-334), last
amended 01 April 2015. Available at: http://
http://laws-lois.justice.gc.ca/eng/regulations/sor-96-334/ (last
accessed 18 June 2015).
- Footnote 73
-
Curt Lewis News-Flight Safety Information No. 143, 17 July 2014 and No. 157, 31 July 2014.
- Footnote 74
-
Percentage of infant and child passenger loads may be higher for
these operators in comparison to air carriers operating in southern
regions of Canada, as they serve northern communities where travel in
and out is mainly by air.
- Footnote 75
-
J. Skills Rasmussen, “Rules, knowledge; signals, signs, and symbols, and other distinctions in human performance models,” IEEE Transactions on Systems, Man and Cybernetics, 13 (1983).
- Footnote 76
-
NAV CANADA, Canada Air Pilot, Alternate weather minima, pp. 28-29.
- Footnote 77
-
Operations Specification 100 (Op Spec 100), Part IV – Authorization of GPS-based instrument approaches are approved by TC.
- Footnote 78
-
Perimeter SA227 Standard Operating Procedures, Section 2 Normal Operations, 2.20 Approach Briefing, p.2-12.
- Footnote 79
-
Transport Canada, TP 2076 – Instrument Procedures Manual (4th edition, November 1997), Section 4.6.3(d).
- Footnote 80
-
From a recent TSB blog article, referencing the Resolute Bay,
Nunavut, controlled flight into terrain/unstable approach occurrence
(TSB Aviation Investigation Report A11H0002). Blog available at:
http://www.bloguebst-tsbblog.com/2014/03/28/one-unstable-approach-many/#.VW8V_nrD-70
(last accessed 18 June 2015).
- Footnote 81
-
Transport Canada, Advisory Circular (AC) 700-016 (2010), Compliance with Regulations and Standards for Engine-Inoperative Obstacle Avoidance.
- Footnote 82
-
Transport Canada, Advisory Circular (AC) 700-016 (2010), Compliance with Regulations and Standards for Engine-Inoperative Obstacle Avoidance.
- Footnote 83
-
Fairchild, SA227-AC Airplane Flight Manual, Performance chart, Figure 4G-4, p. 4G-5 8AC, equipped with McCauley propellers.
- Footnote 84
-
Ibid., Figure 4H-7, p. 4H-9 8AC.
- Footnote 85
-
Flight Operational Quality Assurance (FOQA) is a voluntary safety
program designed to improve aviation safety through the proactive use of
flight recorded data. Operators use these data to identify and correct
deficiencies in all areas of flight operations. Properly used, FOQA data
can reduce or eliminate safety risks, as well as minimize deviations
from regulations.
- Footnote 86
-
Transport Canada, Staff Instructions, SI SUR-001, Issue
No. 4 came into effect on 17 Novembe 2010, and governed the surveillance
activities described here. It was superseded by Issue No. 5 on
28 June 2013. This document refers to Issue No. 4, unless otherwise
specified.
- Footnote 87
-
A process comprising research and an on-site review of one or more
components of a safety management system or other regulated areas of an
enterprise. Transport Canada, Staff Instructions, SI SUR-001, Issue No. 4, Definitions, p. 8.
- Footnote 88
-
An in-depth review of an enterprise process utilized to produce an output. Transport Canada, Staff Instructions, SI SUR-001, Issue No. 4, Definitions, p. 9.
- Footnote 89
-
Transport Canada, Aviation Safety Oversight, Staff Instructions, SI-SUR-001, Issue No. 4, Sections 13.1 and 15.1.
- Footnote 90
-
An organization’s procedures dictate the specific steps an
individual should take to accomplish a task. They operationalize the
philosophy and policies by indicating how work will be carried out.
(Transportation Safety Board of Canada, A Guide to Investigating for Organizational and Management Factors, Version 1, February 2002.)
- Footnote 91
-
An organization’s practices represent what actually happens in
day-to-day operations. In an ideal world, practices and procedures would
be identical. However, in reality, practices may differ from procedures
for a number of reasons. (Transportation Safety Board of Canada, A Guide to Investigating for Organizational and Management Factors, Version 1, February 2002.)
- Footnote 92
-
A hazard is a condition that could cause or contribute to an
aircraft incident or accident. Transport Canada, Aviation Safety
Oversight, Staff Instructions, SI SUR-001, Issue No. 4, Definitions. The Canadian Transportation Accident and Safety Board Act
defines accident as an occurrence that results directly from the
operation of an aircraft, (i) a person is killed or sustains a serious
injury.
- Footnote 93
-
Canadian Aviation Regulations (CAR) 704.33(1)(d) Apron and
cabin safety procedures; Transport Canada, Advisory Circular
(AC) 700-014 Passenger Seating Requirements and Accessible Air
Transportation, Section 4.0 Emergency Exit Seats (4)(g).
- Footnote 94
-
Merriam-Webster Online Dictionary [online]. Available at:
http://www.merriam-webster.com/dictionary/frustration (last accessed 18
June 2015).
- Footnote 95
-
A.J. Maule, G.R.J. Hockey and L. Bdzola, 2000, “Effects of
time-pressure on decision-making under uncertainty: changes in affective
state and information processing strategy,” Acta Psychologica, 104, pp. 283–301.
- Footnote 96
-
A.N. Stephens and J.A. Groeger, 2011, “Anger-congruent behavior transfers across driving situations,” Cognition & Emotion, 25(8), pp. 1423-1438.
- Footnote 97
-
T. Jay, 2000, Why we curse, Philadelphia: John Benjamins.
- Footnote 98
-
T. Jay, 2009, “The utility and ubiquity of taboo words,” Perspectives on Psychological Science, 4(2), pp. 153-161.
- Footnote 99
-
Circadian rhythm timing (circadian dip): fatigue will increase
slightly in the middle of the afternoon and significantly during the
circadian rhythm trough between 22:30 and 04:30 body time.
- Footnote 100
-
Acute reductions in the quantity of sleep are normally considered
remarkable when they are at least 30 minutes in duration. Reductions in
the quality of sleep result from awakenings or other significant changes
to the normal textbook pattern of sleep due to such things as changes
to the time the person goes to bed or wakes up, arousing sleep
environments (e.g., noisy bunk rooms), food choices (e.g., caffeine,
alcohol) or mental stress. Qualitative sleep reductions are normally
considered remarkable when the amount of deep sleep is curtailed to less
than the required 10 to 20% or rapid eye movement (REM) sleep is
curtailed to less than the required 15 to 20% but the total sleep time
may remain unchanged.
- Footnote 101
-
Crew Resource Management (CRM) Standing Group, Crew Resource Management, Royal Aeronautical Society, London, United Kingdom, 1999.
- Footnote 102
-
Federal Aviation Administration, Crew Resource Management Training, 2004, Advisory Circular AC 120-51E.
- Footnote 103
-
Commercial Air Service Standards (CASS) 725.124(39) Crew Resource Management Training, Advisory Circular (AC) 120-51E.
- Footnote 104
-
D. Maurino, Coordinator, Flight Safety and Human Factors Programme, Threat and Error Management
(TEM), – International Civil Aviation Organization (ICAO), Canadian
Aviation Safety Seminar, Vancouver, British Columbia, 18-20 April 2005.
- Footnote 105
-
A. Merritt and J. Klinect, 2006, Defensive Flying for Pilots: An Introduction to Threat and Error Management, The University of Texas Human Factors Research Project. The LOSA Collaborative.
- Footnote 106
-
A Satisfactory Intent assessment is assigned if the stakeholder has
proposed action that, if implemented in full, will substantially reduce
or eliminate the safety deficiency. Associated recommendations are
A00-06 and A07-03.
- Footnote 107
-
A. Gupta, “Trans-Cockpit Authority Gradient in Flying Training: A Case Report,” Indian Journal of Aerospace Medicine, 48(1), 2004.
- Footnote 108
-
K.A. Wilson, J.W. Guthrie, E. Salas and W.R. Howse, 2010, “Team process.” In J.A. Wise, V.D. Hopkin and D.J. Garland (Eds.), Handbook of Aviation Human Factors, Second Edition. Boca Raton, Florida: CRC Press, pp. 9-1 to 9-22.
- Footnote 109
-
A. Merritt and J. Klinect, 2006, Defensive Flying for Pilots: An Introduction to Threat and Error Management, The University of Texas Human Factors Research Project. The LOSA Collaborative.
- Footnote 110
-
D. Maurino, Coordinator, Flight Safety and Human Factors Programme, Threat and Error Management
(TEM), – International Civil Aviation Organization (ICAO), Canadian
Aviation Safety Seminar, Vancouver, British Columbia, 18-20 April 2005.
- Footnote 111
-
The Line Operations Safety Audits (LOSA) Archive is a database
containing observers’ narratives and coded observations from all
25 participating airlines that have conducted a LOSA with the LOSA
Collaborative (from 2002 to 2006). Results from different airlines are
pooled to derive industry averages.
- Footnote 112
-
Transport Canada, Advisory Circular (AC) 302-009.
- Footnote 113
-
International Civil Aviation Organization (ICAO), Document 9613, Performance-based Navigation Manual, Volume 1, Concept and Implementation Guidance, Explanation of terms.
- Footnote 114
-
Flight Safety Foundation, Flight Safety Digest, “Killers in
Aviation: FSF Task Force Presents Facts About Approach-and-landing and
Controlled-flight-into-terrain Accidents,”
November-December 1998/January-February 1999. Available at:
http://www.skybrary.aero/bookshelf/books/1542.pdf (last accessed
18 June 2015).
- Footnote 115
-
J.M. Smith, D.W. Jameson and W.F. Curtis, “Inspiring the Decision to Go Around,” AeroSafety World, June 2013.
- Footnote 116
-
Transport Canada, Air Carrier Advisory Circular No. 0161.
- Footnote 117
-
“Safety experts advise: use the go-around option,” Aviation International News, August 2013.
- Footnote 118
-
Skybrary article “Flying a Manual Go-around” [online]. Available at:
http://www.skybrary.aero/index.php/Flying_a_Manual_Go-around (last
accessed on 18 June 2015)
- Footnote 119
-
“Safety experts advise: use the go-around option,” Aviation International News, August 2013.
- Footnote 120
-
Skybrary article “Go-around Decision Making” [online]. Available at:
http://www.skybrary.aero/index.php/Go-around_Decision_Making (last
accessed 18 June 2015).
- Footnote 121
-
T. Jay 2009, “The utility and ubiquity of taboo words,” Perspectives on Psychological Science, 4(2), pp. 153-161.
- Footnote 122
-
Transport Canada, Instrument Procedures Manual, TP 2076 (4th edition, November 1997), Section 4.6.3(d).
- Footnote 123
-
International Civil Aviation Organization (ICAO), Annual Report of
the ICAO Council: 2013. Available at:
http://www.icao.int/annual-report-2013/Pages/default.aspx (last accessed
18 June 2015).
- Footnote 124
-
Transport Canada, Transportation in Canada 2013, TP 14816. Available
at:
https://www.tc.gc.ca/media/documents/policy/Transportation_in_Canada_2013_eng_ACCESS.pdf(last
accessed 18 June 2015).
- Footnote 125
-
National Transportation Safety Board (2010). Safety Recommendations A-10-121 through -123.
- Footnote 126
-
United Airlines Flight 232-Sioux City, IA 1989; US Air Flight
1016-Charlotte, NC 1994; Continental Flight 267-Severe turbulence 1995;
American Airlines Flight 903-Inflight upset 1997; Southwest Airlines
Flight 2809-Severe turbulence 2008; General Aviation occurrence, Butte,
MT 2009.
- Footnote 127
-
V. Gowdy and R. DeWeese, The performance of child restraint devices in transport airplane passenger seats, Federal Aviation Administration (FAA) Office of Aviation Medicine, Report No. DOT/FAA/AM-94/19. September 1994.
- Footnote 128
-
T. Gibson, K. Thai and M. Lumley, Child restraint in Australian commercial aircraft, Aviation safety research grant report B2004/0241: February 2006.
- Footnote 129
-
European Aviation Safety Agency (EASA.2007.C.28), Study on Child Restraint Systems,
TÜV Rheinland Kraftfahrt GmbH, Team Aviation, November 2008. Available
at:
http://easa.europa.eu/rulemaking/docs/research/Final%20Report%20EASA%202007.C.28.pdf
(last accessed 18 June 2015).
- Footnote 130
-
National Transportation Safety Board (NTSB) (2010). Safety
Recommendations A-90-078, A-93-106, A-93-107, A-93-108, A-93-109, A-10-122,
and A-10-123.
- Footnote 131
-
K. Poland and N.M. Marshall, A Study of General Aviation Accidents Involving Children in 2011, National Transportation Safety Board (NTSB), Washington, D.C., United States.
- Footnote 132
-
National Transportation Safety Board (NTSB) (2010). Safety Recommendations A-10-121 through -123.
- Footnote 133
-
United Airlines Flight 232-Sioux City, IA 1989; US Air
Flight 1016-Charlotte, NC 1994; Continental Flight 267-Severe
turbulence 1995; American Airlines Flight 903-Inflight upset 1997;
Southwest Airlines Flight 2809-Severe turbulence 2008; General Aviation
occurrence Butte, MT, 2009.
- Footnote 134
-
European Aviation Safety Agency (EASA.2007.C.28), Study on Child Restraint Systems,
TÜV Rheinland Kraftfahrt GmbH, Team Aviation, November 2008, pp. 49-51.
Available at:
http://easa.europa.eu/rulemaking/docs/research/Final%20Report%20EASA%202007.C.28.pdf
(last accessed 18 June 2015).
- Footnote 135
-
The European Aviation Safety Agency (EASA) study refers to CRS as a
Child Restraint System tested and approved for motor vehicles held in
place with the vehicle restraints. Child Restraint Device (CRD) is
referred to as a CRS used in an aircraft and held in place with the
provided aircraft restraints.
- Footnote 136
-
Federal Aviation Administration (FAA), AC No. 120-88A, Preventing
Injuries Caused by Turbulence, 19 January 2006. Available at:
https://www.faa.gov/regulations_policies/advisory_circulars/index.cfm/go/document.information/documentID/99831
(last accessed 18 June 2015)
- Footnote 137
-
International Civil Aviation Organization (ICAO), Annual Report of
the ICAO Council: 2013. Available at:
http://www.icao.int/annual-report-2013/Pages/default.aspx (last accessed
18 June 2015).
- Footnote 138
-
Transport Canada, Transportation in Canada 2013, TP 14816. Available
at:
https://www.tc.gc.ca/media/documents/policy/Transportation_in_Canada_2013_eng_ACCESS.pdf
(last accessed 18 June 2015).
- Footnote 139
-
International Civil Aviation Organization (ICAO) working paper of
the Assembly – 38th Session Technical Commission, Agenda Item 31:
Aviation Safety – Emerging Issues, Child Restraint.
A38-WP/287, TE/130, 12/9/13. Available at:
http://www.icao.int/Meetings/a38/Documents/WP/wp287_en.pdf (last
accessed 18 June 2015).
- Footnote 140
-
International Civil Aviation Organization (ICAO) working paper of
the Assembly – 38th Session Technical Commission, Agenda Item 31:
Aviation Safety – Emerging Issues, Child Restraint.
A38-WP/99, TE/31, 22/8/13.
- Footnote 141
- A point that an aircraft must overfly at a defined height before manoeuvring for final approach.